
Retrospective assessment of factors associated with readmission in a large psychiatric hospital in Guangzhou, China
2014-12-09 07:00YanlingZHOURobertROSENHECKSomaiaMOHAMEDNiFANYupingNINGHongboHE
上海精神医学 2014年3期
Yanling ZHOU, Robert A. ROSENHECK, Somaia MOHAMED, Ni FAN, Yuping NING, Hongbo HE*
•Original article•
Retrospective assessment of factors associated with readmission in a large psychiatric hospital in Guangzhou, China
Yanling ZHOU1, Robert A. ROSENHECK2, Somaia MOHAMED2, Ni FAN1, Yuping NING1, Hongbo HE1*
psychiatric inpatients, readmission, length of stay, survival analysis, mental health law, China
1. Introduction
Severe mental illnesses are often characterized by a chronic relapsing course that may require repeated hospital admissions. A substantial body of research in high-income countries (where most inpatient admissions are voluntary) has identified several potential predictors of readmission following a psychiatric hospitalization:poor access to post-discharge outpatient services,younger age, more severe clinical diagnosis (e.g.schizophrenia or bipolar disorder), lack of supportive significant others (being unmarried, divorced, or widowed), medication non-adherence, and poor access to adequate housing.[1-4]One study in the United States found reduced readmissions among individuals whose index admission was court-ordered.[5]Several large studies conducted during the period of de-institutionalization when many public psychiatric hospitals in high-income countries were closed or down-sized found that as the number of total psychiatric beds decreased the average length of inpatient admissions decreased and the rates of readmission increased.[6-8]In the 1990s – after three decades of deinstitutionalization and decreasing average lengths of stay -- 37 to 53% of discharged hospital psychiatric patients in the United States were readmitted within 12 months of their last discharge.[9]One-year readmission rates reported for patients with bipolar I disorder range from 41 to 60%[10,11]and those for patients diagnosed with schizophrenia are about 50%.[6,12]
There have been relatively few studies about psychiatric readmission rates in low- and middle-income countries (LMICs). In China per capita availability of psychiatric beds is much lower than in high-income countries but the lengths of stay are, paradoxically,longer.[13]One possible explanation for this may be that almost all psychiatric admissions are involuntary; in the vast majority of cases the decision to admit a patient to a psychiatric hospital and the decision to discharge the patient from the hospital is made by the patients’guardians, most often family members. Patients are frequently kept in the hospital longer than they might choose if the decision was theirs to make. Thus patients who get admitted to the limited number of available beds are more likely to have prolonged stays and more likely to have family members directly involved in the process of admission and discharge, both of which may reduce the risk of re-hospitalization.
The stipulations of China’s first national mental health law that took effect in May 2013[14]now require that all psychiatric admissions and discharges, other than those in which the individual is an imminent danger to self or other, be voluntary; that is, the patient himself or herself must agree to admission and can decide when he or she wants to be discharged. This major change will take several years to fully implement but it is expected that it will result in a significant decrease in the average length of stay at psychiatric hospitals. The unanswered question of importance to health planners is whether or not the expected decrease in length of stay will be associated with a corresponding increase in readmission rates. To help understand the relationship of length of stay to readmission rates (and to lay down a baseline prior to full implementation of the new mental health law) the current study uses recent administrative data from Guangzhou Psychiatric Hospital (GPH) – one of the largest public psychiatric hospitals in the country – to determine the factors that are associated with one-year readmission rates.
2. Methods
This retrospective study used electronic admissions data from the Guangzhou Psychiatric Hospital, China’s oldest (established in 1898) and one of its largest psychiatric hospitals. This 1900-bed hospital accounts for approximately 70% of all inpatient psychiatric beds in Guangzhou, which is the third largest city in China with a population of 13 million.
2.1 Sample
The identification of patients included in this analysis is shown in the flowchart in Figure 1. Data extracted from the hospital’s electronic admission records covered the period up to December 31, 2013, allowing for one year post-discharge data collection for each patient who had been discharged prior to December 31, 2012.All discharges of patients with a primary psychiatric diagnosis based on the International Classification of Diseases, 10th Revision (ICD-10) between January 1, 2011 and December 31, 2012 in which the index admission had lasted for less than one year (i.e.,excluding chronic care patients) were considered. A total of 4553 discharges following admissions of less than one year occurred in 3455 separate patients over this two-year enrollment period. Subsequent analyses were based on the FIRST discharge (the ‘index’ discharge) of each of these 3455 patients that occurred during the enrollment period. Readmissions that occurred more than one day after the index discharge (i.e., excluding those who were immediately readmitted the next day) and within one year of the index discharge were identified. Among these patients 2979 (86.2%) had no readmissions that occurred more than one day and less than one year after the index discharge and 476 (13.8%)had one or more readmissions that occurred more than one day and less than one year after the first index discharge. The subsequent analyses compared patients who did and did not have one or more readmissions in the year following the index discharge.
This study was a retrospective review of electronic hospital records that did not include disclosure of confidential patient information so it was exempted from full review by the hospital’s ethics review board and written informed consent was not required.
2.2 Measures
Socio-demographic information collected on identified patients was based on the situation at the time of the index admission, that is, the admission that lasted less than one year and resulted in the first discharge of the patient during the two-year enrollment period.Data collected included age, gender, marital status,employment status, relationship with primary caregiver(spouse/partner, parent/child, brother/sister, other relationships), and type of medical insurance (insurance for public servants and state employees, insurance forurban workers and residents, and no insurance [i.e.,self-pay]). Clinical data recorded included the discharge diagnosis at the time of the index discharge (using ICD-10 categories), the duration of the index admission, and the number of past psychiatric hospitalizations (at other hospitals included). The primary outcome measure was days from index discharge (i.e., the first discharge during the enrollment period) to the first readmission at the Guangzhou Psychiatric Hospital. We also recorded the total number of inpatient psychiatric days at the Guangzhou Psychiatric Hospital during the 365 days after the index discharge.

Figure 1. Identification of study patients
2.3 Statistical Analyses
Data analysis proceeded in several steps. First bivariate comparisons were made between patients who did and did not have one or more readmission within one year of the index discharge, using chi square tests for categorical variables, student’s t-test for continuous variables and Wilcoxon rank tests for medians of non-normally distributed variables. For multi-level variables,multiple comparison follow-up tests were used to compare pairs of subgroups if the overall analysis showed significant differences between the groups.
Proportional hazard ratios were used to examine predictors of time to first readmission to the Guangzhou Psychiatric Hospital within one year of the index discharge; not being rehospitalized over this period was defined as censored data. In this analysis length of index admission was classified into 6 categories (with 20 days or less as the reference category) and number of previous psychiatric hospitalizations was categorized into 4 categories (with no prior hospitalizations as the reference category).
In the subgroup of patients who had experienced a readmission, linear regression was used to identify factors associated with the total duration of readmission(s) in the year following the index discharge. The duration of readmission(s) was nonnormal with a strong skew to the right, so the square root transformation of the original data was used in this analysis.
Finally, we repeated the survival analysis and regression analysis adding a term representing theinteraction of the length of the index admission and the number of previous hospitalizations. This additional term makes it possible to determine whether or not a history of extensive and prolonged hospitalization moderates the relationship of the length of the index admission on one-year readmission or on total time of readmission.
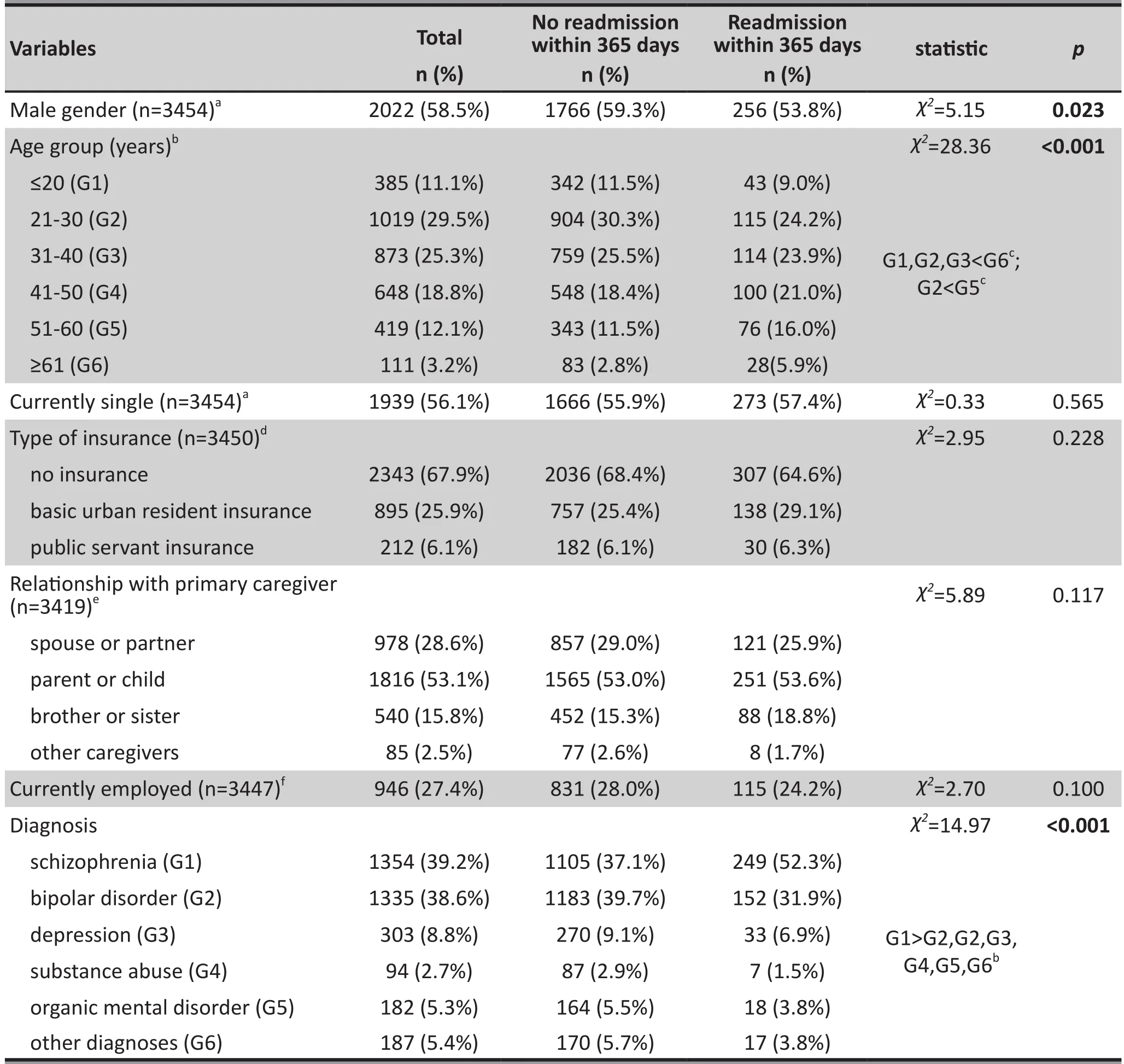
Table 1. Sociodemographic characteristics of 3455 patients discharged from Guangzhou Psychiatric Hospital between January 1, 2011 and December 31, 2012
All data were analyzed using SPSS version 13.0.(SPSS Inc., Chicago, IL, USA). An alpha of p<0.05 was considered statistically significant.

Table 2. Service use of patients with and without readmission within 1 year of index discharge (n=3455)
3. Results
Among the 3455 patients included in the analysis 476(13.8%) were rehospitalized one or more times at the Guangzhou Psychiatric Hospital within one year of the index discharge. As shown in Table 1, compared to those who were not readmitted, patients who were readmitted within one year of the index discharge were significantly less likely to be male, significantly older and significantly more likely to have a discharge diagnosis of schizophrenia than any other diagnosis. There were,however, no significant differences between the two groups of patients in marital status, type of medical insurance, type of primary caregiver, or employment status.
As shown in Table 2, for the majority of patients(52%), the index hospitalization was their first hospitalization. The patients who were readmitted over the 1 year follow-up period were significantly more likely to have two or more prior admissions than those who were not readmitted over the follow-up period.The median duration of the index admission was also significantly longer in the readmitted group than in the non-readmitted group (67 v. 42 days).
Among the 476 patients who were readmitted, 161(33.8%) were readmitted once and 315 (66.2%) were readmitted two times or more over the year of follow-up. One-quarter of those who were readmitted were readmitted within one month of the index discharge.The mean and median number of total days in hospital over the year (combining the different readmissions)were 90.4 days and 68 days, respectively. (Table 2)
Table 3 shows the results of the proportional hazards analysis of the risk of readmission. The bivariate analysis found no significant relationship betweenreadmission and gender, age, marital status, type of medical insurance, type of caregiver, employment status, diagnosis, or duration of index admission.The only factor that was significantly related to the occurrence of a readmission within one year of the index discharge was the number of prior hospital admissions. Patients who had 2 prior admissions were 3.2-fold more likely to be readmitted than those without a prior admission, and those with 3 or more prior admissions were 5.2-fold more likely to be readmitted. This relationship is shown graphically in the survival analysis in Figure 2.

Table 3. Hazard ratio for readmission within 365 days after discharge: Cox proportional hazards model (n=3455)
Table 4 shows the results of the multiple linear regression analysis of the factors associated with the total duration of readmission over the year of follow-up in the 476 individuals who were readmitted.The factor that had the strongest effect on the duration of readmission was the duration of the index hospitalization, longer index hospitalizations were associated with longer readmission times over the subsequent year. One other factor had a weakrelationship with time of readmission: compared to persons without medical insurance those with the basic urban resident insurance were likely to be readmitted longer during the 1 year follow-up.

Figure 2. Time to readmission in patients with mental disorders in the year following an index psychiatric discharge stratified by the different numbers of prior psychiatric hospitalizations

Table 4. Multiple linear regression model of total hospital days in the year after index discharge among the 476 patients who were readmitted in the year after the index dischargea
Addition of the interaction term of the length of the index admission and the number of prior admissions to the survival analysis for time to readmission and to the multiple regression analysis of the total time of readmission did not affect the results, in both cases the interaction term was not statistically significant.
4. Discussion
4.1 Main findings
This study examined correlates of readmission for psychiatric hospitalization within one year of discharge from the largest psychiatric hospital in Guangzhou, China and found that only 13.8% of patients were readmitted one or more times within a year of discharge. The only factor that was significantly associated with risk of readmission was the number of prior admissions.Among those who were readmitted, the main factor that was related to the total time of readmission over the year was the duration of the index admission –longer index admissions were associated with longer periods of readmission in the year after discharge.
The characteristics of the patients in this sample are similar to those reported from elsewhere in China and substantially different from those reported in the United States and other high-income countries. The median length of admission of 46 days in our study was within the range of 43 to 336 days reported for other psychiatric hospitals in China,[15-17]but it was much longer than the 4 to 27 day mean length of stay reported in high-income countries.[7,18,19]Similarly, the relatively low one-year readmission rate of 13.8% seen in this study is similar to rates reported from other centers in China[19,20]but much lower than the 16 to 42.5%readmission rates reported from the United States.[21,22]The short psychiatric hospitalizations and frequent readmissions seen in many high-income countries are the result of a long process of de-institutionalization and down-sizing of psychiatric hospitals that started in the 1960s and 1970s,[3,23,24]and that was associated with substantial reductions in total psychiatric bed availability.
China’s new mental health law, which went into effect in May, 2013, specif i es that patients have the right to discharge themselves from the hospital unless they are determined to be a danger to themselves or others.As a result, it is widely anticipated that the length of stay will decline as patients elect to leave the hospital earlier than previously. This has led to the legitimate concern that as length of stay falls, readmission rates may rise and, by implication, outcomes will be poorer, similar to the trajectory observed in high-income countries. But,unlike in high-income countries, there is no strong deinstitutionalization movement in China, so it is likely that shorter hospital stays, ongoing economic development and increasingly comprehensive insurance coverage will be accompanied by increased psychiatric bed availability and expanded community-based services.[13]Thus, it is certainly possible that shorter lengths of stay in China will not be accompanied by more readmissions and generally poorer outcomes, particularly if the expansion of community-based services envisioned in the new mental health law is realized. Our study provides one piece of evidence to support this conclusion– readmission rates and duration of subsequent hospitalization do not increase with shorter index hospitalizations. But more comprehensive, prospective studies that follow the changes as voluntary admission becomes the rule in Chinese psychiatric hospitals will be needed confirm this interpretation.
One other factor that could affect readmission rates which is quite different between China and most high-income countries is the much higher degree of involvement of patients’ families in the care of the patients, a role that is codified in the new mental health law. In our study, 98% of the identified sample had a family caregiver who was involved in the decision to hospitalize the patient. There aren’t directly comparable figures from high-income countries but only 43% of the patients with schizophrenia who participated in the large Clinical Antipsychotic Trials of Intervention Effectiveness (CATIE) study in the United States had family members who participated in the family burden part of the study; a replication of the CATIE study at the Guangzhou Psychiatric Hospital identified family participants in 92% (140/152) of the cases.
Most, but not all, patients with serious mental illness in China live with family members. In this study 68% of the patients had no medical insurance and 72% were unemployed, so the economic burden on the family of providing care and treatment for the patient is substantial. In most cases family members also manage the patients’ medication and instigate outpatient visits when symptoms exacerbate. This may change as the increased mobility of the population,particularly from rural to urban settings, leads to more isolated individuals, but for the foreseeable future family involvement in the care of persons with serious mental illness will probably remain a major factor in the relatively low rates of rehospitalization. However, if the frequency and duration of hospitalizations decreases it is likely that the burden of caring for the mentally ill individuals borne by the co-resident family members will increase, perhaps to the point where they will ‘give up’ on the patient and be more inclined to place them in the chronic care psychiatric institutions run by the Ministry of Civil Affairs. But this may not be the outcome if high-quality, community-based mental health services that can provide families with practical help in caring for the patients are made available.
4.2 Limitations
This study had several limitations. First, our data on rehospitalization are limited to admissions to Guangzhou Psychiatric Hospital. While it is possible that we underestimated the readmission rate and that some of the patients were readmitted to other hospitals,the Guangzhou Psychiatric Hospital accounts for 70%of all psychiatric beds in Guangzhou and is the most likely site of readmission, particularly among patients who have already been admitted to the hospital. To assess the magnitude of the potential bias introduced in the results because of this problem, were-analysed the data on the subsample of patients with at least one previous admission to the Guangzhou Psychiatric Hospital (n=1662) – those least likely to have sought rehospitalization elsewhere. The main results in this subsample were the same as those in the full sample:number of previous hospitalizations was significantly related to risk of rehospitalization but duration of index admission was not. We conclude that this limitation does not seriously bias our results.
Second, this is a retrospective, observational study in which many potentially important clinical characteristics were not measured. Multivariable analysis was used to adjust for past hospitalization, one potential indicator of severity, but a richer array of covariates would be desirable. Measures of severity of psychopathology,insight into illness, level of social support,[26]access to community services, premorbid psychosocial functioning, exposure to intense expressed emotion[26],and medication adherence would add to the validity of our analysis. An experimental design with random assignment to different lengths of stay regimes among individual patients or different inpatient wards would be optimal for determining the effects of lowering length of stay on readmission rates, but such a study would be difficult to implement for both ethical and practical reasons.
A third limitation is that we excluded chronic care patients (who were admitted for more than oneyear) and did not do a stratified analysis by diagnosis.It is certainly possible that the pattern of risk factors for readmission and the factors associated with the duration of readmission vary by diagnosis and for persons who have chronic versus acute hospitalizations.Presumably, the patient mix at a hospital will affect the results of such an analysis. So our results may not be representative of hospitals that have substantially different proportions of chronic versus acute admissions or substantially different diagnostic profiles.
A final limitation is that our outcome measures of readmission and post-discharge hospital days do not directly address differences in patients’ clinical status or,perhaps more importantly, in family burden, which has been shown to increase with shorter lengths of stay.[26]In view of the high levels of involvement of families in psychiatric hospital care in China, family burden and its health related consequences deserve special attention as a potential adverse effect of declining lengths of stay of persons with serious mental illnesses.
4.3 Implications
Despite these limitations, this study identified no association between the length of the index admission and either the risk of readmission or the duration of readmission in the year after discharge. It is expected that China’s new mental health law, which allows nonviolent patients to self-discharge, will gradually lead to substantial reductions in China’s relatively long mean duration of psychiatric hospitalization. The concern is that this expected reduction in length of stay will result in higher rates of readmission, poorer long-term outcomes, and increased family burden. Our finding that shorter lengths of stay were not associated with higher rates of readmission provides some reassurance that these negative outcomes will not occur. But prospective studies in other localities with a more comprehensive set of outcome measures (including patient functioning,medication adherence, and family burden) will be needed to monitor the effect of the law both on patients and their families and on the distribution of services between specialized psychiatric hospitals and community-based mental health programs.
Acknowledgements
The authors thank all the investigators for their assistance in this project.
Funding
This study was supported from funding to H.H. from the Chinese National Key Clinical Program in Psychiatry to the Guangzhou Brain Hospital, Guangzhou, China (No.201201001) and from the Guangzhou Municipal Health Bureau (No. 20131A011083). The funding source had no role in the study design, analysis or interpretation of data or in the preparation of the report or decision to publish.
Conflict of interest
The authors declare no conflict of interest.
1. Goodpastor WA, Hare BK. Factors associated with multiple readmissions to an urban public psychiatric hospital. Hosp Community Psychiatry. 1991;42(1): 85-87
2. Baron K, Hays JR. Characteristics of readmitted psychiatric inpatients. Psychol Rep. 2003;93(1): 235-238. doi: http://dx.doi.org/10.2466/PR0.93.5.235-238
3. Figueroa R, Harman J, Engberg J. Use of claims data to examine the impact of length of inpatient psychiatric stay on readmission rate. Psychiatr Serv. 2004.55(5): 560-565. doi:http://dx.doi.org/10.1176/appi.ps.55.5.560
4. Bobier C, Warwick M. Factors associated with readmission to adolescent psychiatric care. Aust NZ J Psychiatry. 2005;39(7): 600-606. doi: http://dx.doi.org/10.1111/j.1440-1614.2005.01632.x
5. Valevski A, Olfson M, Weizman A, Shiloh R. Risk of readmission in compulsorily and voluntarily admitted patients. Soc Psychiatry Psychiatr Epidemiol. 2007;42(11):916-922. doi: http://dx.doi.org/10.1007/s00127-007-0243-7
6. Appleby L, Desai PN, Luchins DJ, Gibbons RD, Hedeker DR.Length of stay and recidivism in schizophrenia: a study of public psychiatric hospital patients. Am J Psychiatry. 1993;150(1): 72-76
7. Lieberman PB, Wiitala SA, Elliott B, McCormick S, Goyette SB. Decreasing length of stay: are there effects on outcomes of psychiatric hospitalization. Am J Psychiatry. 1998;155(7):905-909
8. Heeren O, Dixon L, Gavirneni S, Regenold WT. The association between decreasing length of stay and readmission rate on a psychogeriatric unit. Psychiatr Serv. 2002;53(1): 76-79. doi:http://dx.doi.org/10.1016/j.schres.2006.01.012
9. Strober M, Morrell W, Lampert C, Burroughs J. Relapse following discontinuation of lithium maintenance therapy in adolescents with bipolar I illness: a naturalistic study. Am J Psychiatry. 1990;147(4): 457-461
10. Perlick DA, Rosenheck RA, Kaczynski R, Swartz MS, Canive JM, Lieberman JA. Special section on CATIE baseline data: components and correlates of family burden in schizophrenia. Psychiatr Serv. 2006;57(8): 1117-1125. doi:http://dx.doi.org/10.1176/appi.ps.57.8.1117
11. Segal SP, Burgess PM. Conditional release: a less restrictive alternative to hospitalization. Psychiatr Serv. 2006;57(11): 1600-1606. doi: http://dx.doi.org/10.1176/appi.ps.57.11.1600
12. Weiden P, Aquila R, Standard J. Atypical antipsychotic drugs and long-term outcome in schizophrenia. J Clin Psychiatry.1996;57(Suppl 11): 53-60
13. Qian J. Mental health care in China: providing services for under-treated patients. J Ment Health Policy Econ. 2012;15(4): 179-186
14. Chen HH, Phillips MR, Cheng H, Chen QQ, Chen XD, Fralick D, et al. Mental health law of the People’s Republic of China(English translation with annotations). Shanghai Archives of Psychiatry. 2012;24(6): 305-321. doi: http://dx.doi.org/10.3969/j.issn.1002-0829.2012.06.001
15. Wan YQ, Xie B, Zheng ZP. [Risk factors of 1-year readmission in depression]. Shanghai Jing Shen Yi Xue. 2000;12(3): 146-147. Chinese
16. Ren CR. [Effect in length of stay of schizophrenia patients].Zhongguo Jian Kang Xin Li Xue Za Zhi. 2002;10(1): 33-34.Chinese. doi: http://doi.med.wanfangdata.com.cn/10.3969/j.issn.1005-1252.2002.01.019
17. Wang CJ, Zhu SR. [Gender differences in the effect, diagnosis and length of stay of mental illness]. Sichuan Jing Shen Wei Sheng. 2004;17(1): 43. Chinese. doi: http://doi.med.wanfangdata.com.cn/10.3969/j.issn.1007-3256.2004.01.025
18. Pertile R, Donisi V, Grigoletti L, Angelozzi A, Zamengo G,Zulian G, et al. DRGs and other patient-, service- and arealevel factors influencing length of stay in acute psychiatric wards: the Veneto Region experience. Soc Psychiatry Psychiatr Epidemiol. 2011;46(7): 651-660. doi: http://dx.doi.org/10.1007/s00127-010-0231-1
19. Zhang YB. Predictors of re-hospitalization over a twoyear follow-up period among patients with schizophrenia enrolled in a community management program in Chengdu,China. Shanghai Archives of Psychiatry. 2012;24(1):7. doi: http://doi.med.wanfangdata.com.cn/10.3969/j.issn.1002-0829.2012.01.004
20. Guo JH, Gao CA, Gao H, Pu WJ. [Retrospective study on readmission of female psychiatric patients]. Zhongguo Min Kang Yi Xue. 2007;19(3): 101-102. Chinese.doi: http://doi.med.wanfangdata.com.cn/10.3969/j.issn.1672-0369.2007.03.008
21. Albrecht JS, Hirshon JM, Goldberg R, Langenberg P, Day HR,Morgan DJ, et al. Serious mental illness and acute hospital readmission in diabetic patients. Am J Med Qual. 2012;27(6):503-508. doi: http://dx.doi.org/10.1177/1062860612436576
22. Lin HC, Tian WH, Chen CS, Liu TC, Tsai SY, Lee HC. The association between readmission rates and length of stay for schizophrenia: a 3-year population-based study. Schizophr Res. 2006;83(2-3): 211-214. doi: http://dx.doi.org/10.1016/j.schres.2006.01.012
23. Mechanic D, McAlpine DD, Olfson M. Changing patterns of psychiatric inpatient care in the United States, 1988-1994.Arch Gen Psychiatry. 1998;55(9): 785-791. doi: http://dx.doi.org/10.1001/archpsyc.55.9.785
24. American Hospital Association. AHA Hospital Statistics,1993–1994. Chicago, Ill, AHA. 1993
25. Thompson A, Shaw M, Harrison G, Ho D, Gunnell D, Verne J. Patterns of hospital admission for adult psychiatric illness in England: analysis of Hospital Episode Statistics data.Br J Psychiatry. 2004;185: 334-341. doi: http://dx.doi.org/10.1192/bjp.185.4.334
26. Roick C, Heider D, Kilian R, Matschinger H, Toumi M,Angermeyer MC. Factors contributing to frequent use of psychiatric inpatient services by schizophrenia patients. Soc Psychiatry Psychiatr Epidemiol. 2004;39(9): 744-751. doi:http://dx.doi.org/10.1007/s00127-004-0807-8
27. Rosenheck R, Cramer J, Jurgis G, Perlick D, Xu WC, Thomas J,et al. Clinical and psychopharmacologic factors influencing family burden in refractory schizophrenia. The Department of Veterans Affairs Cooperative Study Group on Clozapine in Refractory Schizophrenia. J Clin Psychiatry. 2000;61(9): 671-676
2014-02-27; accepted: 2014-06-03)

Yanling Zhou obtained her Bachelor’s degree in clinical medicine from Sun Yat-Sen University School of Medicine in 2007 and her Master’s degree from Guangzhou Medical University in 2014. She has been working as an attending psychiatrist at Guangzhou Psychiatric Hospital since 2007. Her main research interest is in mental health services.
回顾性评估中国广州一家大型精神病医院再住院的相关因素
周燕玲,Rosenheck RA,Mohamed S,范妮,宁玉萍,何红波
精神科住院患者,再住院,住院天数,生存分析,精神卫生法,中国
Background:Most psychiatric inpatients in China are involuntarily admitted by their families, resulting in relatively long admissions and relatively low readmission rates. However, this pattern may change after implementation of China’s new national mental health law (promulgated in 2013), which restricts involuntary psychiatric admissions to the small proportion of mentally ill individuals who are a danger to self or others.Aim:Assess the factors associated with readmission rates of psychiatric inpatients in Guangzhou, China.Methods:A retrospective analysis of data from the Guangzhou Psychiatric Hospital, one of the largest psychiatric hospitals in China, used Cox regression models to evaluate the relationship between age, gender,diagnosis, marital status, employment status, relationship with the primary caregiver, type of medical insurance, length of stay of the index admission, and the number of previous admissions to estimate the risk of readmission over the year following discharge. Multivariate regression is used to assess factors associated with the total time of readmission during the year of follow-up.Results:Among 3455 patients admitted from 1 January 2011 to 31 December 2012 who had a mean(sd) length of stay of 65.7 (66.3) days, 476 (13.8%) were readmitted one or more times within one year of discharge. After considering all potential predictors of readmission in a multivariate survival analysis,the number of previous hospitalizations prior to the index admission was the only statistically significant predictor of readmission. The only factor that was significantly related to the total time of readmission was the duration of the index admission.Conclusion:Shorter length of stay was not associated with increased readmission rates in patients admitted to a large public psychiatric hospital in southern China. This suggests that the expected decrease in the length of psychiatric inpatient admissions that is likely to occur when, based on China’s new regulations, most patients are admitted voluntarily may not lead to increased rates of readmission. Prospective studies with a more comprehensive set of outcome measures (including patient functioning, medication adherence, and family burden) are needed to monitor the effect of the law on patients and on the distribution of mental health services.
http://dx.doi.org/10.3969/j.issn.1002-0829.2014.03.005
1Neuropsychiatric Research Institute, Guangzhou Psychiatric Hospital, Guangzhou Medical University, Guangzhou, China2Department of Psychiatry, Yale University School of Medicine, New Haven, United States
* correspondence: hongbo_he@yeah.net
A full-text Chinese translation of this article will be available at www.saponline.org on July 25, 2014.
背景:中国大多数精神科住院患者是由家人强制性入院,导致住院时间相对较长和再次住院率相对较低。然而,这种模式随着新颁布的中国精神卫生法(颁布于2013年)可能发生变化,该法限定了强制性精神科入院为那些对自己或他人产生危险的小部分精神疾病患者。目标:评估中国广州精神科住院患者再次住院率的相关因素。方法:对从中国最大的精神病医院之一——广州市精神病医院收集来的数据进行回顾性分析,使用Cox回归模型评估年龄、性别、诊断、婚姻状况、就业状况之间的关系,与主要照顾者的关系、医疗保险、指标住院的时间、以往的入院次数之间的关系,进而评估出院后一年内再住院的风险。使用多因素回归分析来评估随访一年中再次住院总时间的相关因素。结果:2011年1月至2012年12月31日间3455例住院患者的平均住院时间(标准差)为65.7(66.3)天,476(13.8%)名患者出院后一年内再入院一次或多次。在将再入院所有可能的预测因素进入多因素生存分析后,指标住院前的以往住院次数是再次住院的唯一有统计学意义的预测因子。与再住院总时间显著相关的唯一因素是指标住院的长短。结论:缩短住院时间并没有增加中国南方一家大型公立精神病院的患者再住院率。这表明,根据中国的新法规,大部分病人自愿入院时不仅不会导致再次住院率的增加,可能还会出现预期的精神病患者的住院时间的缩短。前瞻性研究将需要结合更全面的结果评估(包括患者功能,服药依从性,和家庭负担)来监测精神卫生法对患者和精神卫生服务分布的影响。
猜你喜欢
中国民间疗法(2021年10期)2021-07-22
世界最新医学信息文摘(2021年12期)2021-06-09
医学与法学(2020年3期)2020-09-18
中国卫生(2015年2期)2015-11-12
中国卫生(2015年6期)2015-11-08
中国健康心理学杂志(2015年6期)2015-09-05
中国司法鉴定(2015年4期)2015-02-28
中国卫生(2015年3期)2015-01-22
中国卫生(2014年8期)2014-11-12
安徽医药(2014年9期)2014-03-20
- 上海精神医学的其它文章
- Neuroimaging studies of depressive disorders in China since 2000
- Two-year prospective case-controlled study of a case management program for community-dwelling individuals with schizophrenia
- Changes in behavior and in brain glucose metabolism in rats after nine weeks on a high fat diet: a randomized controlled trial
- Retrospective assessment of the prevalence of cardiovascular risk factors among homeless individuals with schizophrenia in Shanghai
- Opportunities and challenges for promoting psychotherapy in contemporary China
- Case report of comorbid alcohol-induced psychotic disorder and Madelung’s disease