
Cytokines predict virological response in chronic hepatitis B patients receiving peginterferon alfa-2a therapy
2020-06-17 05:54WenKangFuJieCaoNingNingMiChongFeiHuangLongGaoJinDuoZhangPingYueBingBaiYanYanLinWenBoMeng
World Journal of Clinical Cases 2020年11期
Wen-Kang Fu, Jie Cao, Ning-Ning Mi, Chong-Fei Huang, Long Gao, Jin-Duo Zhang, Ping Yue, Bing Bai,Yan-Yan Lin, Wen-Bo Meng
Wen-Kang Fu, Jie Cao, Ning-Ning Mi, Chong-Fei Huang, Long Gao, Wen-Bo Meng, The First Clinical Medical School, Lanzhou University, Lanzhou 730000, Gansu Province, China
Jie Cao, Laboratory Department of the First Hospital of Lanzhou University, Lanzhou 730000,Gansu Province, China
Jin-Duo Zhang, Ping Yue, Bing Bai, Yan-Yan Lin, Wen-Bo Meng, Special Minimally Invasive Surgery Department, The First Hospital of Lanzhou University, Lanzhou 730000, Gansu Province, China
Wen-Bo Meng, Institute of Genetics, School of Basic Medical Sciences, Lanzhou University,Lanzhou 730000, Gansu Province, China
Wen-Bo Meng, Institute of Hepatopancreatobiliary of Gansu Province, Lanzhou 730000, Gansu Province, Chinao
Wen-Bo Meng, Key Laboratory of Biotherapy and Regenerative Medicine of Gansu Province,Lanzhou 730000, Gansu Province, China
Abstract
Key words: Chronic hepatitis B; Peginterferon-alpha-2a; Cytokine/chemokine; CXCL9;Interferon-inducible protein 10; Thymus and activation-regulated chemokine
INTRODUCTION
Despite the development of a highly effective and safe vaccine over 30 years ago,chronic hepatitis B virus (HBV) infection remains a global major public health problem, and at least 257 million people are chronically infected with HBV worldwide[1]. Approximately 887000 chronic hepatitis B (CHB) patients die annually from complications associated with the disease, including cirrhosis, hepatocellular carcinoma, and liver failure[1-10]. Effective antiviral drugs inhibit replication and reduce the risks of CHB complications[11]. Host and viral factors play key roles in the natural history of CHB, the disease activity, and the effectiveness of antiviral therapy[12]. CHB patients generally have an impaired host immune response, which may be associated with a persistent high viral load and subsequent T cell failure[11,13]. At present, the antiviral strategy for CHB mainly lies in the effective suppression of the virus and the recovery of HBV-specific immune responses[12]. Because peginterferon-alpha-2a (PEGIFN) has direct antiviral and immunoregulatory effects, it has become one of the first choice drugs for the treatment of CHB[14]. Antiviral treatment with PEG-IFN effectively inhibits HBV replication and may lead to seroconversion of hepatitis B e antigen (HBeAg), clearance of hepatitis B surface antigen (HBsAg), normalization of alanine aminotransferase (ALT) levels, and histologic improvement[11]. If patients achieve an IFN induced virological response, they may achieve long-term therapeutic effects while reducing the risks of cirrhosis and HCC[11,14]. When patients with CHB receive PEG-IFN treatment, there is no guarantee of a sustained virology response,and studies show that only 30% of patients benefit from this treatment[15]. Since PEGIFN has the properties of immune regulation, the host immune status may affect the efficacy of PEG-IFN in the treatment of CHB[11,12]. Several studies in recent years have shown that cytokines and chemokines may play a potential role in chronic viral hepatitis[12,16,17].
Cytokines play an important role in immunity, and they directly inhibit viral replication and indirectly determine the predominant pattern of the host immune response[18]. Chemokines are a group of small cytokines that induce the migration of circulating white blood cells to sites of inflammation or injury and enhance the phagocytosis abilities of inflammatory cells[19]. Due to the highly complex control of cytokine secretion, the interactions between cytokines, and with their receptors, are widely spread in numerous regulatory networks[19]. Screening multiple biomarkers can clarify the immune mechanism of HBV infection and predict the response to antiviral therapy. Moreover, a study has demonstrated that T cell responses and circulating cytokines are associated with HBV replication and liver function.Interleukin (IL)-10, IL -12, and IL -21 play crucial roles in the immune clearance stage;thus, they are related to the seroconversion of HBeAg[11,16,18,19]. Nevertheless, the relationship between multiple cytokines and chemokines and the responses to PEGIFN therapy in patients with CHB has not previously been clarified.
In this study, we analyzed the serum levels of cytokines in CHB patients receiving PEG-IFN treatment and responses to the therapy. Forty-six cytokines, including macrophage inflammatory protein 1d (MIP-1d), CXCL9, CXCL6, IP10, and TARC, in serum samples of CHB patients were simultaneously tested. The predictive value of the cytokines for the responses to PEG-IFN was also assessed.
MATERIALS AND METHODS
Serum samples
In total, 78 serum samples were prospectively collected with written informed consent from 26 CHB patients undergoing PEG-IFN therapy between August 2018 and June 2019. All patients were positive for serum HBsAg for more than 6 mo, and patients receiving PEG-IFN therapy fulfilled the treatment criteria for CHB according to the American Association for the Study of Liver Disease treatment guidelines,i.e., serum ALT levels > 80 U/L (2 × upper limit of normal) with HBV DNA > 20000 IU/mL in HBeAg positive patients[14]. The patients were treated with 180 μg of PEG-IFN per week for 48 wk. Venous blood samples were drawn from patients with consent at two to four time points as follows: Before PEG-IFN therapy and during PEG-IFN therapy(24 wk and/or 48 wk after initiation of the therapy). The patients were classified as virological responders (VRs) when the serum HBV DNA levels at the 6thmo fter the initiation of the therapy were decreased to less than 2000 IU/mL[20], and the other patients were classified as virological non-responders (NRs). This study was approved by the Institutional Review Board, the First Hospital of Lanzhou University,and complied with the standards of the Declaration of Helsinki and current ethical guidelines. All patients provided written informed consent for participation in the study.
Measurement of cytokine levels
Serum was separated within 2 h of obtaining venous blood samples. If cytokine measurements were not possible on the same day, the samples were immediately stored at -80 °C until the concentrations of cytokines were measured. A Luminex 200 analyzer and Cytokine Array I reagents (Randox, Antrim, United Kingdom) were used to quantify 46 cytokines in the serum, including BCA-1, CTACK, ENA-78,Eotoxin-2, SDF-1a, TARC, TRAIL, TSLP, CCL19, CXCL9, IP-10, EGF, Eotaxin, GRO,IL-8, and MIP-1b. All experiments are measured according to the manufacturer's instructions.
Other assays
The serum HBV DNA levels were assayed using a COBAS Amplicor/COBAS TaqMan HBV test (Roche Diagnostics, Indianapolis, IN, United States) with a limit of detection of 20 IU/mL, according to the manufacturer’s instructions. HBV serologic tests for HBsAg, HBeAg, anti-HBs antibody, and HBeAb were conducted by enzyme immunoassays (AxSYM; Abbott Laboratories, Abbott Park, IL, United States). The levels of serum albumin, ALT, aspartate aminotransferase (AST), and total bilirubin were determined using a Hitachi 7600 analyzer (Hitachi Ltd., Tokyo, Japan) with dedicated reagents (Roche Diagnostics, Mannheim, Germany). The assay was carried out according to the manufacturer's instructions.
Statistical analysis
Values are expressed as the median (ranges) or the mean ± SD when appropriate. The correlations between the serum ALT and chemokine levels were tested by Spearman’s test. The Mann-WhitneyUtest was used to compare a series of continuous variables.The Kruskal-Wallis test and Bonferroni correction were used for multiple comparisons of continuous variables, including cytokine levels between patient subgroups and treatment stages, to compensate for alpha statistical errors. Friedman's test was also performed to compare cytokine levels between paired groups.Friedman's test was carried out to compare the cytokine levels among the paired groups. Categorical variables between the two groups were analyzed for the difference in proportion by Fisher's exact test. The areas under the receiver operating characteristic curves (AUROC) of the cytokines and HBV DNA were calculated to assess their predictive values for virological responses. All statistical analyses were performed using the Statistical Package for Social Sciences (SPSS 17.0 for Windows,SPSS Inc., Chicago, IL, United States), andP< 0.05 was considered statistically significant.
RESULTS
Characteristics of the CHB patients
The characteristics of 26 patients with CHB are summarized in Table 1. The age and male proportions were not different between the VRs (n= 15) and NRs (n= 11). Before peginterferon treatment, there was no difference in serum AST and ALT levels between VRs and NRs, but AST and ALT levels were higher in NRs during and after treatment. Serum HBV DNA levels before, during, and after the therapy were lower in the VRs than in the NRs. Among the VRs, ten (66.7%) demonstrated HBeAg seroconversion during or after the therapy.
Serum levels of cytokines according to treatment phases and therapeutic responses
Serum levels of 46 cytokines in the phases of peginterferon therapy in the VR and NR groups are summarized in Table 2. The levels of all cytokines, with the exception of BCA-1, CTACK, ENA-78, Eotoxin-2, SDF-1a, TARC, TRAIL, TSLP, CCL19, CXCL9, IP-10, EGF, Eotaxin, GRO, IL-8, and MIP-1b, were not statistically significant between the treatment response group and the non-response group before and after treatment.
The levels of CXCL9 and IP10 were higher in the VR group than in the NR group (P= 0.041 and 0.027, respectively). After 24 wk of treatment, CXCL9 and IP10 were significantly lower in the VR group (P= 0.005,P= 0.006), whereas the levels of these two cytokines were not significantly changed according to the phases of the therapy in the NR group (Figure 1A and B). The levels of MIP-1d in the response group at baseline and 24 wk of treatment were higher than those in the NR group (P= 0.036 and 0.041, respectively) (Figure 1C). However, the levels of TARC at baseline and 24 wk in the VRs were lower than those in the NRs (P= 0.016 and 0.021, respectively)(Figure 1D). The level of SDF-1a in the NRs was higher than that in the VRs at 24 wk of treatment (P= 0.032). The CXCL6 level was higher in the VRs than that in the NRs at 24 wk (P= 0.012).
由上述变量的基本描述性统计可以看出,公众满意程度的标准差相对较大,并且其变量值均大于零,结合变量的经济意义及模型求解的需要,我们对公众满意程度的变量值取对数,再进行模型估计。
Correlation between serum ALT and chemokine levels
The serum ALT and 46 chemokine levels were measured at each time point during PEG-IFN treatment for correlation analysis. ALT had positive correlations with the serum BCA-1, SCF, CCL19, CXCL9, CXCL6, and CXCL11 levels (r= 0.526,P= 0.006;r= 0.448,P= 0.022;r= 0.452,P= 0.02;r= 0.588,P= 0.002;r= 0.530,P= 0.005; andr=0.661,P< 0.0001). ALT was inversely correlated with the serum Eotoxin-2, IL-16, IL-8,and MIP-1a (r= -0.517,P= 0.006;r= -0.458,P= 0.019;r= -0.404,P= 0.041; andr= -0.388,P= 0.05).
Predictive value of HBV DNA, HBeAg, and cytokines
The AUROC values of the serum HBV DNA and HBeAg levels measured before peginterferon therapy were 0.879 and 0.964 (P= 0.001,P< 0.001), respectively (Figure 2A). The sensitivity and specificity of the baseline HBV DNA levels in predicting VR were 90.90% and 86.70%, respectively, when the cutoff DNA level was 7.015 IU/mL.The sensitivity and specificity of the baseline HBeAg levels in predicting VR were 100% and 93.30%, respectively, when the cutoff DNA level was 820.95 IU/mL (Figure2A). Moreover, the AUROC value of the baseline TARC levels was 0.77 (P= 0.021) in detecting VR, and the lower TARC level was related to VR. The sensitivity and specificity of the baseline TARC level in discriminating VRs from NRs were 72.70%and 73.30%, respectively, with the cutoff value of 26.52 pg/mL. MIP-1d, CXCL9,CXCL6, and IP10 also had good predictive value. The AUROC values of the serum MIP-1d, CXCL9, CXCL6, and IP10 levels measured before peginterferon therapy were 0.787, 0.799, 0.722, and 0.787 (P= 0.01, 0.01, 0.05, and 0.013), respectively, in predicting VR. The sensitivity and specificity of the baseline MIP-1d, CXCL9, CXCL6, and IP10 levels in predicting VR were 69.20% and 84.60%, 76.90% and 76.90%, 61.50% and 84.60%, and 61.50% and 92.30%, respectively, when the cutoff values were 1662.5 pg/mL, 2840.5 pg/mL, 154.50 pg/mL, and 1332.50 pg/mL, respectively (Figure 2B).The AUROC values of all other cytokines quantified in the serum samples before the therapy were not statistically significant in predicting VR.

Table 1 Baseline characteristics of patients with chronic hepatitis B
DISCUSSION
Liver inflammation due to HBV infection is immune mediated. Acquired immunity and innate immunity are considered related to the pathogenesis of CHB[21]. In this study, we obtained simultaneous measurements of 46 kinds of cytokines in CHB patients to assess the roles of cytokines according to the responses to PEG-IFN, which is a widely used therapeutic agent for the treatment of CHB. However, interferon therapy for CHB remains a clinical challenge. Although successful PEG-IFN therapy can induce a long-lasting response and reduce liver-related complications, the efficacy rate of conventional interferon therapy for 6 mo was only 25% to 40%[22,23]. Therefore,individualized treatment strategies according to pretreatment parameters should be established to identify patients with the highest chance of response. However, there is currently no ideal pre-treatment predictor of VR.
In our study, the serum levels of cytokines changed in the CHB patients during PEG-IFN therapy, and the baseline TARC, MIP-1d, CXCL9, CXCL6, and IP10 levels were strongly correlated with the virological response in patients with CHB. Among these cytokines, high baseline levels of MIP-1d, CXCL9, and IP10 had better prediction of the virological response to interferon therapy. CXCL6, CXCL9, and IP10 are all members of the chemokine ELR-CXC subfamily, in which CXCL9 and IP10 can be induced by IFN-γ[12,24]. These three cytokines are secreted by mononuclear/macrophage T lymphocytes, B lymphocytes, hepatocytes, fibroblasts,etc.CXCL9 and IP10 bind to their co-receptor CXCR3, activate T cells, NK cells,etc, and exert antiviral effects[12,25-27]. Biècheet al[28]reported that CXCL9 and IP-10 were significantly increased in the serum of patients with CHB[28]. A study found a high correlation between high baseline levels of IP10 and hepatitis C virus (HCV) clearance induced by PegIFNα treatment in HCV-infected patients[29]. The baseline levels ofCXCL9 and IP10 were significantly higher in the response group than in the nonresponse group; however, there was a significant decrease in the response group after 24 wk of treatment, and there was no significant difference in the non-response group before and after treatment. Studies have indicated that CXCL9 and IP10 mRNAs were significantly decreased in peripheral blood mononuclear cells of CHB patients after 12-24 wk of PegIFNα treatment, which was similar to the findings in patients with chronic hepatitis C infection[30-32]. According to our study and reports in the literature,the serum levels of CXCL9 and IP10 and the mRNA levels of CXCL9 and IP10 in peripheral blood mononuclear cells decreased in patients who responded to PEG-IFN treatment, which might reflect a reduced hepatic necro-inflammatory activity after treatment. CXCL9 and IP-10 were reported to correlate with hepatic injury during hepatic flares in CHB, and a strong correlation of serum CXCL9 and IP-10 levels with ALT levels was also noted[33]. Our results also showed positive correlations of CXCL6 and CXCL9 with ALT levels (r= 0.530,P= 0.005;r= 0.588,P= 0.002). However, IP-10 was not correlated with ALT, which was different from that in the previous literature and may be related to the relatively few samples tested and individual differences of the hosts. Mac-2-binding protein glycosylation isomer (M2BPGi), also called WFA+-M2BP, is a serum biomarker for assessing liver fibrosis in patients with viral hepatitis[34], and its levels significantly correlated with serum IP-10 levels[35]. A recent study suggested that baseline serum M2BPGi level can be a useful marker in the CHB patients during PEG-IFN therapy[36]. The positive correlations between these parameters may imply that these chemokines have positive impacts on the liver inflammation and HBV control, albeit the relevance was not satisfactory due to the complex interactions between other host and viral factors that contribute to liver inflammation. These findings indicate that CXCL6, CXCL9, and IP10 are associated with hepatic necro-inflammation, and these chemokines are induced and participate in immune responses against HBV infection.
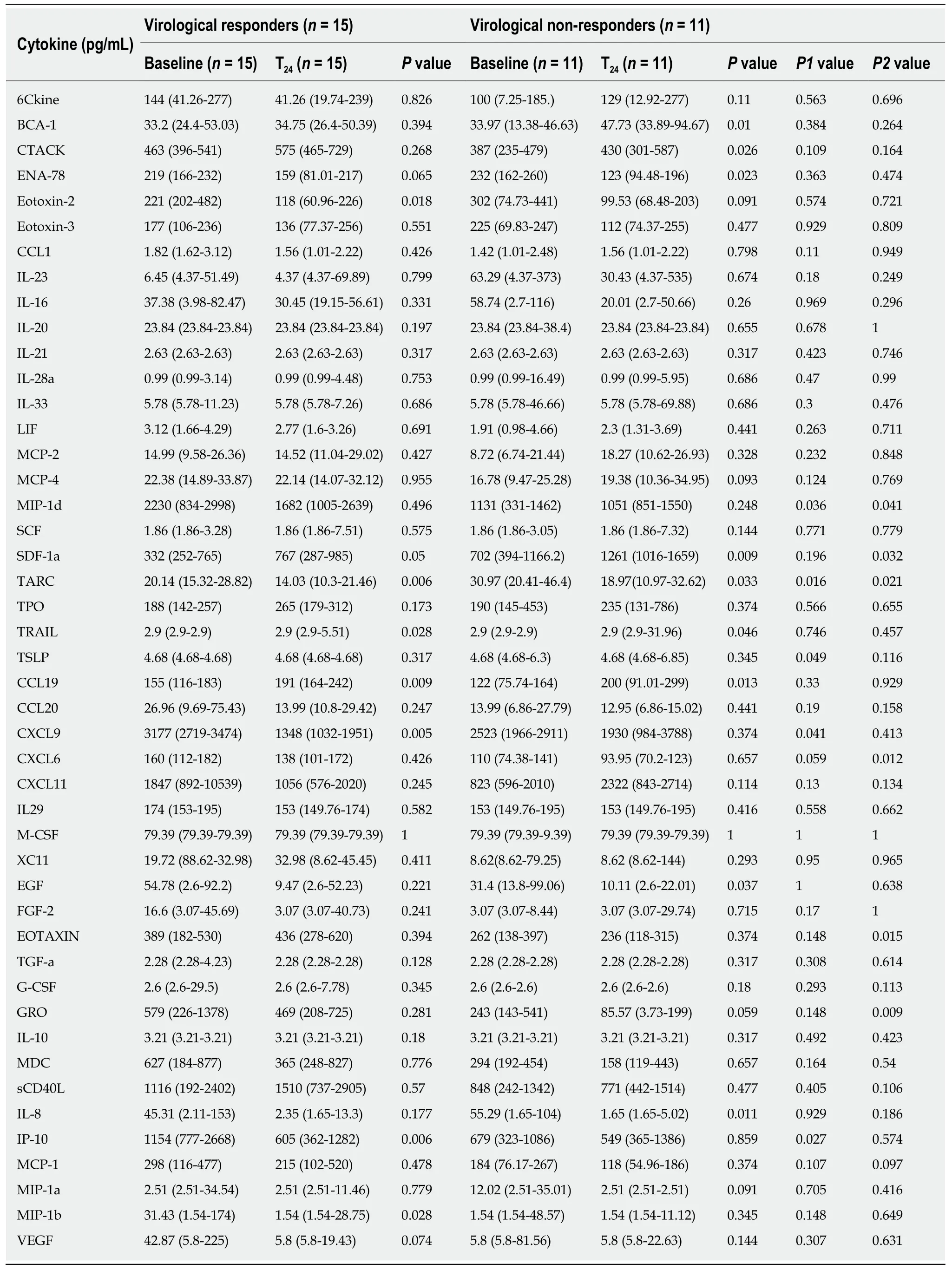
Table 2 Serum levels of 46 cytokines in the phases of peginterferon therapy in the virological responders and non-virological responders group
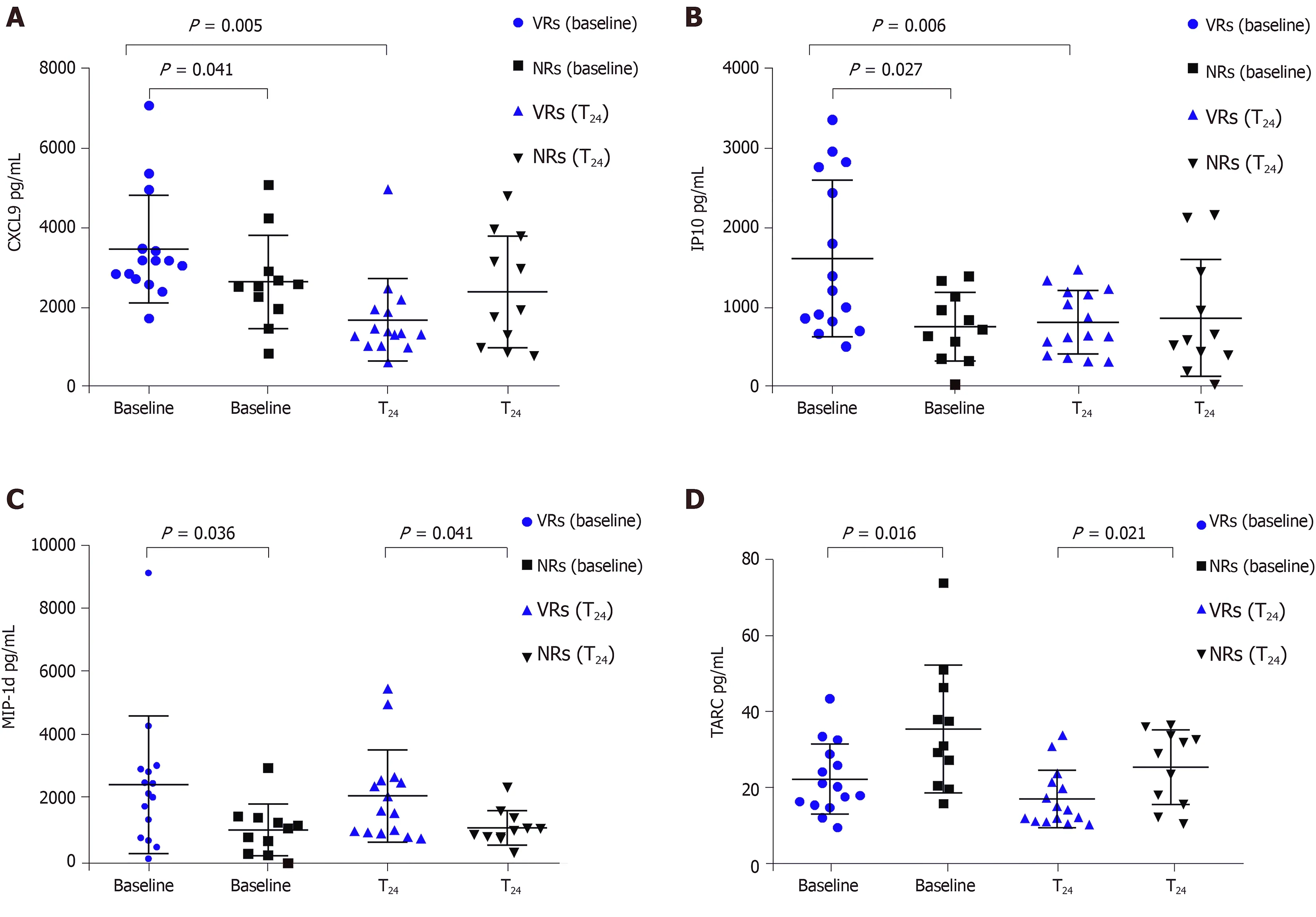
Figure 1 Serum levels of cytokines in chronic hepatitis B patients according to treatment phases and responses to peginterferon α-2a. A: CXC-chemokine ligand 9; B: Interferon gamma-induced protein 10; C: Macrophge inhibitory protein-1 delta; D: Thymus and activation-regulated chemokine. VRs: Virological responders, NRs: Non-virological responders; CXCL9: CXC-chemokine ligand 9; IP10: Interferon gamma-induced protein 10; MIP-1d: Macrophge inhibitory protein-1 delta; TARC: Thymus and activation-regulated chemokine.
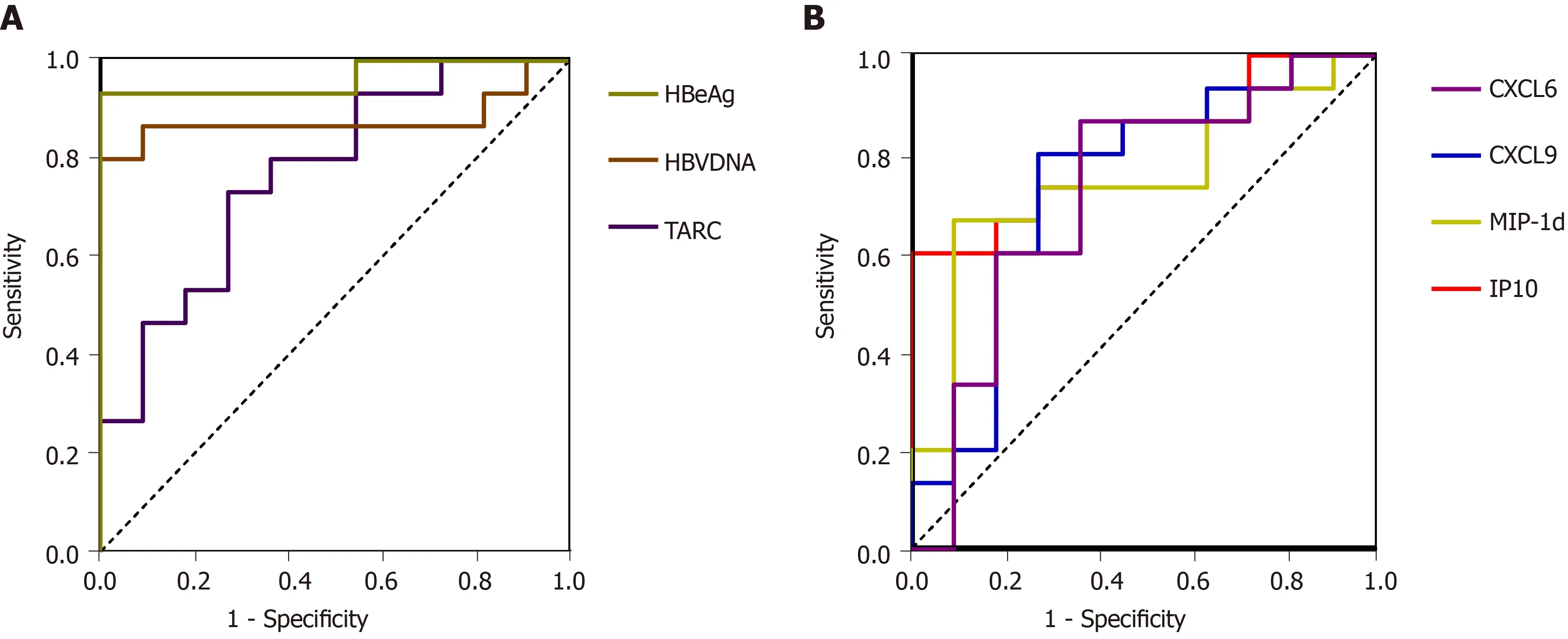
Figure 2 Receiver operating characteristic curves of hepatitis B virus deoxyribonucleic acid, hepatitis B e antigen, and cytokines for predicting virological responses. A: The receiver operating characteristic curves values of the serum hepatitis B virus deoxyribonucleic acid and hepatitis B e antigen levels measured before peginterferon therapy were 0.879 and 0.964, respectively. The sensitivity and specificity of the baseline thymus and activation-regulated chemokine were 72.70% and 73.30%, respectively; B: The sensitivity and specificity of the baseline macrophge inhibitory protein-1 delta, CXC-chemokine ligand 9, CXC-chemokine ligand 6, and interferon gamma-induced protein 10 levels in predicting virological responder were 69.20% and 84.60%, 76.90% and 76.90%, 61.50% and 84.60%, and 61.50% and 92.30%, respectively. HBeAg: Hepatitis B e antigen; HBV: Hepatitis B virus; TARC: Thymus and activation-regulated chemokine; CXCL6: CXCchemokine ligand 6; MIP-1d: Macrophge inhibitory protein-1 delta; IP10: Interferon gamma-induced protein 10.
We also found that TARC in patients with an interferon-treated response was lower than that in the NRs at baseline; however, the level in the response group remained lower than that in the non-response group after 24 wk of treatment. TARC is a member of the CC chemokine group that is constitutively expressed in the thymus and is produced by dendritic cells, endothelial cells, keratinocytes, bronchial epithelial cells, and fibroblasts[37,38]. TARC is a ligand for CCR4, which is predominantly expressed on Th2 lymphocytes, basophils, and natural killer cells[38]. ARC can recruit a large number of Th2 cells, despite the fact that the Th2 cell predominance is to maintain the chronic carrying state of virus infection[39]. Th2 cell activation inhibits both acute and chronic inflammatory reactions[40]. Therefore, the higher expression of TARC in the non-response group treated with interferon is related to the poor prognosis.
MIP-1d/CCL15, a member of the CC chemokine family that is expressed only in the gut and the liver, acts mainlyviathe CC chemokine receptor CCR1[41,42]. MIP-1d was demonstrated to have a chemoattractant role for monocytes, lymphocytes,neutrophils, eosinophils, and dendritic cells. In addition, this molecule plays an important role in the development of inflammatory diseases[41,43]. Our study found that MIP-1d was higher in the response group than in the non-response group at baseline and after 24 wk of treatment. The higher level in the response group than in the non-response group may be associated with better recruitment of T cells in the response group.
CXCL6/GCP-2 is a member of the ELR-CXC chemokines. CXCL6 is mainly secreted by macrophages and epithelial and stromal cells[44]. The receptors of CXCL6 are CXCR1 and CXCR2, and CXCL6 has the functions of regulating immunity, tumor growth, and metastasis, as well as promoting angiogenesis. Liver tissue can express CXCL6, which can induce Kupffer cell, neutrophil, and lymphocyte infiltration in liver inflammation[44,45]. The expression of CXCL6 was elevated in liver inflammation and fibrosis, and in alcoholic hepatitis, CXCL6 levels are elevated and related to the prognosis of patients[45]. In our study, CXCL6 was significantly higher at both baseline and 24-wk in the response group than in the non-response group and showed a significant correlation with ALT.
In conclusion, our results suggest that MIP-1d, CXCL9, CXCL6, IP-10, and TARC have predictive significance in interferon therapy. Cytokines are fundamental molecules in the complex signaling network of cell-mediated immunity. Analyses of the changes in cytokine expression patterns during treatment can help to understand the pathogenesis of CHB and predict treatment responses. However, there were limited subjects in this study, and unfortunately, we could not collect all samples from each patient at all treatment phases. Therefore, the statistical power was not adequate for an assessment of the usefulness of cytokines in monitoring CHB patients. Further large and long-term follow-up studies are required to determine the predictive value of cytokines in CHB patients receiving PEG-IFN treatment. In addition, the differences in these factors between the response and non-response groups and their specific biological roles in HBV infection require further investigation.
ARTICLE HIGHLIGHTS
Research background
Hepatitis B virus (HBV) infection remains a global major public health problem. Chronic hepatitis B (CHB) patients generally have an impaired host immune response, which may be associated with persistently high viral load and subsequent T cell failure. Since peginterferonalpha-2a (PEG-IFN) has direct antiviral and immunoregulatory effects, it has become one of the first choice drugs for the treatment of CHB. PEG-IFN has the properties of immune regulation,and the host immune status may affect the efficacy of PEG-IFN in the treatment of CHB.
Research motivation
Recently, many studies have shown that cytokines and chemokines may play a potential role in chronic viral hepatitis. We aimed to determine the correlation between cytokine/chemokine expression levels and response to PEG-IFN treatment in patients with CHB.
Research objectives
Our main purpose was to analyze the serum levels of cytokines in CHB patients receiving PEGIFN treatment and responses to the therapy, and to assess the predictive value of the cytokines for the responses to PEG-IFN.
Research methods
In total, 78 serum samples were prospectively collected with written informed consent from 26 CHB patients undergoing PEG-IFN therapy. A Luminex 200 analyzer and Cytokine Array I reagents were used to quantify 46 cytokines in the serum. The serum HBV DNA levels were assayed using a COBAS Amplicor/COBAS TaqMan HBV test, and HBeAb was measured by enzyme immunoassay.
Research results
A total of 26 patients (17 males and 9 females; mean age, 28.8.3 ± 4.161 years in virological responders group, and 27.82 ± 4.446 years in virological non-responders group) were enrolled in the study. The monokine induced by INF-γ (CXCL9) and serum interferon-inducible protein 10(IP-10) levels at baseline were higher in the virological responders than in the non-virological responders and decreased during treatment. The CXCL9, IP-10, macrophage inflammatory protein 1d (MIP-1d), and thymus and activation-regulated chemokine (TARC) baseline levels exhibited the expected effects for interferon treatment. The area under the receiver operating characteristic curve values of CXCL9, IP-10, MIP-1d, and TARC for predicting the virological response were 0.787, 0.799, 0.787, and 0.77 (P= 0.01, 0.013, 0.01, and 0.021), respectively.
Research conclusions
In conclusion, our results suggest that MIP-1d, CXCL9, CXCL6, IP-10, and TARC have predictive significance in interferon therapy. Cytokines are fundamental molecules in the complex signaling network of cell-mediated immunity. Analyses of the changes in cytokine expression patterns during treatment can help to understand the pathogenesis of CHB and predict treatment responses.
Research perspectives
Further large and long-term follow-up studies are required to determine the predictive value of cytokines in CHB patients receiving PEG-IFN treatment. Besides, the differences in these factors between the response and non-response groups and their specific biological roles in HBV infection require further investigation.
猜你喜欢
新世纪智能(数学备考)(2021年9期)2021-11-24
外语学刊(2021年1期)2021-11-04
语数外学习·高中版中旬(2021年12期)2021-03-09
计算机技术与发展(2020年9期)2020-11-26
语数外学习·高中版上旬(2020年8期)2020-09-10
新高考·高一数学(2016年10期)2017-07-06
考试周刊(2016年90期)2016-12-01
人间(2016年27期)2016-11-11
医学理论与实践(2012年4期)2012-12-09
中学生数理化·八年级数学人教版(2008年6期)2008-09-05
 World Journal of Clinical Cases2020年11期
World Journal of Clinical Cases2020年11期
- World Journal of Clinical Cases的其它文章
- Tumor circulome in the liquid biopsies for digestive tract cancer diagnosis and prognosis
- Isoflavones and inflammatory bowel disease
- Cytapheresis for pyoderma gangrenosum associated with inflammatory bowel disease: A review of current status
- Altered physiology of mesenchymal stem cells in the pathogenesis of adolescent idiopathic scoliosis
- Association between liver targeted antiviral therapy in colorectal cancer and survival benefits: An appraisal
- Peroral endoscopic myotomy for management of gastrointestinal motility disorder