
Art making and expressive art therapy in adult health and nursing care:A scoping review
2021-02-28 09:49HeliVrtioRjlinReginSntmkiFischerPmelJokisloLisbethFgerstr
Heli Vrtio-Rjlin ,Regin Sntm¨ki-Fischer ,Pmel Jokislo ,Lisbeth FgerstrÖm ,c
a Health Sciences,Åbo Akademi University,Vasa,Finland
b Bachelor of Healthcare/Nursing,Novia University of Applied Sciences,Åbo,Finland
c Health Sciences,University of South-Eastern Norway,Kongsberg,Norway
Keywords:Adult Aged Art making Art therapy Health care Nursing care Person-centered care
ABSTRACT Objectives:While receptive art engagement is known to promote health and wellbeing,active art engagement has not been fully explored in health and nursing care.This review is to describe the existing knowledge on art making and expressive art therapy in adult health and nursing care between 2010 and 2020.Methods:Relevant studies and grey literature were searched and identified between March 17 and April 10,2020 from EBSCO,CINAHL,Medline and ERIC databases and a general Internet search.Following data charting and extraction,the data (n=42 papers) were summarized and reported in accordance with PRISMA-ScR guidelines.Results:In the included papers,both art making and expressive art therapy were seen in different health care and nursing contexts:yet not the home care context.The emphasis of art activities were group activities for chronically or terminally ill residents,adults aged 65 years or older.A focus on personal narrative was often seen,which may explain why art activities appear to be linked to acknowledging and building new strengths and skills,making meaning of experiences,personal growth,symptom alleviation,and communication; all used to foster collaboration between patients,patients’ near-ones and health care professionals.Conclusions:Art activities appear to be suitable for every context and can promote personcenteredness and the measurement of nursing outcomes,and they should be considered an essential part of health and nursing care,nursing education and care for health care personnel.
What is known?
·Receptive art engagement is known to promote health,selfworth,accomplishment and patients’,patients’ near-ones’ and health care professionals’ social engagement.
·Nursing is often described as an art,and health care professionals and patients engaging in art and/or craft making together as fellow human beings has been shown to have a positive effect for both parties and can help diminish power hierarchies.
·Humanistic expressive art therapy is characterized by the work process itself,exposure to a wide range of materials,and the employment of a variety of techniques in therapeutic intervention,used to help individuals explore their hidden feelings in a supportive setting.
What is new?
·Art activities appear to be mainly organized as part of research or general projects,not as systematic health or nursing care interventions,even though most art activity types can be undertaken alone without any special skills and/or significant material investments.
·Health care professionals should be encouraged to use art activities intentionally,to get to know each persons’ narratives,because the meaning of the person’s experiences is a vital part of evidence-based nursing art and person-centered care.
·Whether art activities should be overseen by a nurse or a professional art therapist can be argued:art activity outcomes can be related to nursing goals and nursing outcomes,which could be measured through observations of patients’art activities and narratives linked to such activities.
1.Introduction
The arts play a significant role in modern health sciences,and they can be used to skillfully interpret emotions,helping one better understand oneself and others [1].In health and nursing care,in addition to a focus on the signs and symptoms of a health problem or an illness,there should be a focus on potential (skills or strengths)and satisfaction(areas,actions and activities that bring a satisfying feeling).Seen more broadly,this should include personcentered health and nursing care interventions [2]and nonpharmacological interventions using art [3].The arts and creative expression have been shown to promote health,self-worth,accomplishment,and social engagement [3]:for patients,patients’ near-ones and health care professionals [4].
The arts can be defined as music,performance arts (theatre,dance),the visual arts,the literary arts(novel-writing,poetry,other forms of text) and the huge range of applied arts [5].The arts can play an integrative role in facilitating lifelong learning,seen as discovering and building new skills and making meaning of experience,because through art one’s past and present thoughts can be combined.Arts engagement can be either receptive (attending concerts,theatre,reading)or active(art making)[6].One does not need to be an artist or have any special skills to express oneself through art making; the most important thing is an open attitude to creativity in everyday life.This allows one to give oneself and others a chance to interact with and be touched by art and to vary the pattern of everyday life.
Creative expression is characterized by active participation in the process of bringing something new into existence:the production or performance of art or the creation of an original idea,perspective or process [7].Creative activities facilitate selfexpression,social interaction,communication,sensory stimulation and emotional relief,in a failure-free environment [8].Art therapy can also serve as a link through which individuals can explore past and present experiences,review one’s life,cope with,adjust to,and adapt to age-related changes,be supported during an emotional crisis,or be given care related to physical loss (for example,loss of an organ,memory or mobility)[9].Art therapy has especially been applied in oncologic,dementia and mental care.Art therapy must be overseen by an art therapist,and time must be given to verbally processing the feelings arising from the art experience.Conversely,art making need not be overseen by an art therapist.Consequently,it is a practical alternative to art therapy and can still serve as a basis for a person-centered approach to health and nursing care.
2.Background
2.1.The arts and art making in health and nursing care
In a Health Evidence Network synthesis report from the World Health Organization [2],researchers found evidence that the arts play a major role in the promotion of good health,the prevention of a range of mental and physical health conditions,and the treatment or management of conditions arising across the life-course.For people with acute conditions,access to the arts in the hospital and/or in the community can help improve experience and outcomes in emergency care and rehabilitation.For people with chronic conditions,access to the arts can support mental health,physical functioning and social and emotional well-being.The arts can even be used to address complex challenges for which there are no current health care solutions.For both those living at home or in an institution,the arts can enrich one’s life.Enjoying the arts by,for example,visiting an art gallery,is not likely to produce lasting effects.However,even for those with severe dementia,enjoyment can be derived from the arts [10].Valuable social and emotional support in palliative care and bereavement can also be provided through the arts[2].Furthermore,the arts have even been used to investigate brain alterations in artists arising from frontotemporal dementia [11]and dementia-related delirium and confabulation[12].
Engagement in creative expression can also lead to improved outcomes for patients[3,4,8].While art making can be perceived as too demanding,art crafting (craft making) can be more easily accepted.Craft making is defined as a form of production that requires some skill,personal insight and practice and encompasses any of the manual arts:for example,weaving,knitting,felting,quilting,embroidery,needlework,basket-weaving,leatherwork,woodwork,copper-tooling or metalcraft.Craft making as purposeful activity has for decades traditionally been used in occupational therapy and/or rehabilitation[13].Art and/or craft making have been shown to alleviate symptoms of,for example,depression and fatigue during chemotherapy[14],stress and anxiety[15]and can help repair or maintain function in diverse parts of the body or be used to motivate patients to regain function so that they can participate in society again.Health care professionals and patients engaging in art and/or craft making together as fellow human beings has also been shown to have a positive effect for both parties and can help diminish power hierarchies [13].Furthermore,the implementation of arts programs in medical education or health care organizations has been found to improve students’ and personnel’s mental health and well-being and reduce stress and burnout [4].
Storytelling or individual narratives can be considered creative expressions [16].Stories illuminate the person,allowing a glimpse of him/herself in decades past.Through stories one not only gains information about the person being cared for but can also facilitate the retrieval of experiences,resources,values and wishes.Reminiscing about one’s own history or home is essential to a personcentered approach,not only in elderly care [17]but also in situations that presuppose a need for identity reconfiguration and restored self-esteem,such as disruption,divorce or chronic illness.By asking a person to,“Tell me a story about…”,one can uncover information critical to the planning of effective care consistent with the person’s desires and goals [18].Used as an alternative to interpreting how a person perceives his/her body image during a health problem or illness,individual narrative in the form of asking a person to draw or tell a story can also be used to help improve self-worth[19].Individual narratives in patient education can also take the form of illustrated stories,comic strips [12]or social theatre [20].
Creative expression not only enhances a person’s health and well-being,it also enriches communities.The arts and culture have played a crucial role in building cities and towns,fostering unique neighborhoods,and binding communities together[4].The arts are also linked to positive effects in building intergenerational bonds[21].Engagement with the arts can help address social determinants of health,for example through the development of social cohesion,reduction of loneliness and social isolation and building of individual and group identity.The arts are also effective in reaching people who are either less likely to seek health care or who experience more barriers when seeking it and therefore may have a higher risk of adverse health outcomes [4].
2.2.Expressive art therapy in health and nursing care
Humanistic expressive art therapy is unlike the analytic or medical model of art therapy,where art is used to diagnose,analyze and “treat” people [22].It is characterized by the work process itself,exposure to a wide range of materials,and the employment of a variety of techniques in therapeutic intervention [9].Expressive art therapy can help individuals explore their hidden feelings in a supportive setting [17].Used to facilitate growth and healing and expressed through various art forms (movement,drawing,painting,sculpting,music,writing,sound,and improvisation) [22],expressive art therapy can be considered a process of discovering oneself through any art form that emerges from an emotional depth.The creative connection can be considered a spiral of activities,through which layers of inhibition are removed.Through a person-centered approach in expressive art therapy,the therapist’s role -being empathic,open,honest,congruent,and caring -can be emphasized.Expressive art therapy is not used to analyze or solve a problem,nor is it about(striving for)perfection;it is a path to self-expression and a way to release one’s feelings.
Art therapists are qualified health professionals who have undertaken postgraduate studies in art therapy [22].They must also register with and be authorized by national supervisory boards,for example,with the National Supervisory Authority for Welfare and Health in Finland (https://www.valvira.fi/web/en/healthcare/professional_practice_rights).Without full qualifications and registration,a person cannot act as an art therapist nor practice art therapy; “art therapist” is a protected title [22].This is important,because it allows one to discern between a professional art therapist and a“non-professional”who is merely facilitating art making.
In one review[23],art therapy was found to be effective but not typically more effective than standard therapy.The researchers in that review failed to define the type of art therapy explored or in what/which context(s),but did note that expressive art therapy was excluded.In another review in which the researchers limited inclusion to papers in which art therapy was noted as the specific intervention [24],researchers found that art therapy can lead to positive treatment outcomes for the populations (all ages) and settings (schools,outpatient clinics,day treatment centers and treatment centers,hospitals and nonclinical settings) included in that review.
2.3.Nursing art and person-centered care
Certain nursing theorists have explored the artistic aspects of nursing.In accordance with Jean Watson,the union between the nurse and the person(individual or community level)is an artistic act and an expression of caregiving,which is unique and personal[25].Also other nursing theorists such as Martha Rogers,Faye Glen Abdellah,Ernestine Wiedenbach and Rosemarie Rizzo Parse define nursing as an art [26].As a concept,the art of nursing can be defined as,“the intentional creative use of oneself,based upon skill and expertise,to transmit emotion and meaning to another.It is a process that is subjective and requires interpretation,sensitivity,imagination,and active participation” [27].Nursing is an aesthetic knowledge(art),where the nurse must make use of his/her internal creative resources to transform others’ experiences.The action,behaviors,attitudes and interactions occurring in a given narrative reveal the transformation,performance and creativity inherent to the narrative [28].Aesthetic knowing,seen as the nurse’s perception of the person and the person’s needs,is related to the nurse’s“artful” performance of manual and technical skills.The nurse’s perception of what is significant in the person’s behavior is revealed through the pattern underlying the nurse’s aesthetic knowing.Accordingly,one can maintain that the pattern of aesthetic knowing is focused on particulars rather than universals[29].
Virginia Henderson argued that,“the nurse’s goal is to assist the patient to become complete,whole,or independent” [30].While nurses follow a physician’s therapeutic plan,individualized care is seen and realized through the nurse’s creativity in planning for care.In good,person-centered care,nurses actively seek and foster patient narratives or other creative patient expressions to gain mutual understanding of not only symptoms and problems but also strengths and areas of satisfaction.In person-centered care,the“whole patient”,seen as a psychosocial and existential person,is taken into consideration in health and nursing care.This is shown as respect for the personal narratives that reflect a person’s sense of self,lived experiences and relationships and the recognition of this respect through the safeguarding of a partnership in shared decision-making and in meaningful activities in a personalized environment [31-33].In person-centered care,storytelling or narratives (for example,expressed through art making,crafting or art therapy activities) and the art of nursing are interwoven.To foster such care,nurses need not be art therapists and patients need not be artists.However,the nurses should know how art making and expressive art therapy can be used (contexts,types,to whom,by whom,eventual challenges) and what are the outcomes that could be expected.
3.Aim
The aim of this scoping review was to describe the existing knowledge on art making and expressive art therapy in adult health and nursing care.The research questions were:
-How is art making used in adult health and nursing care?
-How is expressive art therapy used in adult health and nursing care?
-What are the outcomes of the different art making and/or expressive art therapy activities in adult health and nursing care?
4.Methods
To describe the existing knowledge[34]on art and art therapy in adult health and nursing care,a scoping review method was chosen.Scoping reviews constitute a relevant method used to map evidence in complex research areas.Arksey and O’Malley found that while systematic reviews tend to include a focus on a welldefined research question and design,scoping reviews are used to explore a broader research question and include studies that reflect a greater variety of designs.The steps in a scoping review include the identification of research question(s),identification of relevant studies,selection of studies,charting of data,and summarization and reporting of results[35].The PRISMA-ScR checklist was used to guide the reporting in this review[34].
4.1.Search strategy and information sources
As a first step,the identification of research questions occurred.This was followed by the identification of relevant studies and grey literature,which included theoretical papers,statement papers and practice-oriented development reports.Between March 17 and April 10,2020,searches of the EBSCO,CINAHL,Medline and ERIC databases were conducted.A general Internet search (Google and Google Scholar)was also undertaken to identify grey literature.The MeSH search terms included“art”AND“nursing”as subject terms.As the main topic of interest,the search term(major heading)“art”was set to include:art as art making,expressive art therapy,paintings,creativeness,creativity,nursing as art,museums,photography,music therapy,drawings,and literature.The search term (major heading) “nursing” was set to include all aspects of professional nursing and health care provided by the search engine(f.eg.nursing as art,nursing education,nursing care,nursing practice,caring,nursing as profession,nursing science;psychiatric nursing,oncology nursing,occupational health care,public health care and so on).
4.2.Eligibility criteria
The eligibility criteria included full-text published or to-bepublished,peer-reviewed studies,theoretical papers and grey literature with a focus on art making or expressive art therapy with adults (>18 years) in the context of health and nursing care between January 2010 and December 2020.Studies and papers were to be written in English or Finnish,and grey literature had to be either a statement paper or a practice-oriented development report.The time period for this study was chosen to complement already-existing reviews on art therapy:prior to 1999 [18],1999-2007 [24]and a 2008-2013 review of the efficacy of art therapy[36].During the search,no other reviews of art making or expressive art therapy in health and nursing care were found.
4.3.Charting and analysis of data
During the screening of potentially relevant papers for inclusion,117 references were identified through the electronic database searches and general Internet search (Fig.1).Level one testing included title and abstract screening,during which conference papers without actual research or project results,commercial websites marketing art therapy,papers with a focus on neurological processing during art or art therapy experiences (considered irrelevant,n=11)and duplicates(n=33)were excluded.Relevant papers were then retained for full-text review in level two testing and reviewed by the first author (HVR).In this phase,papers without a free full-text version (n=31) were excluded due to economic reasons.
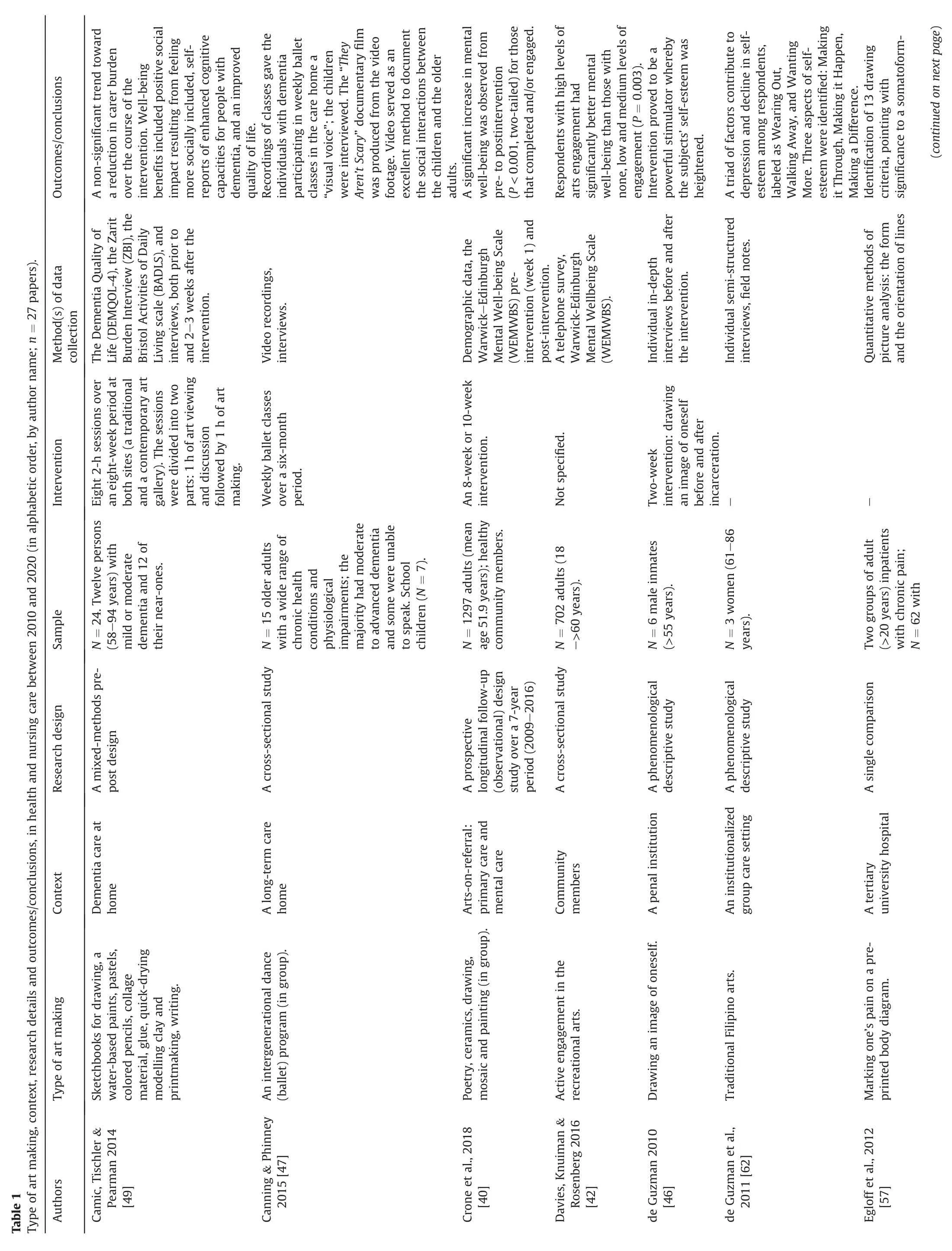
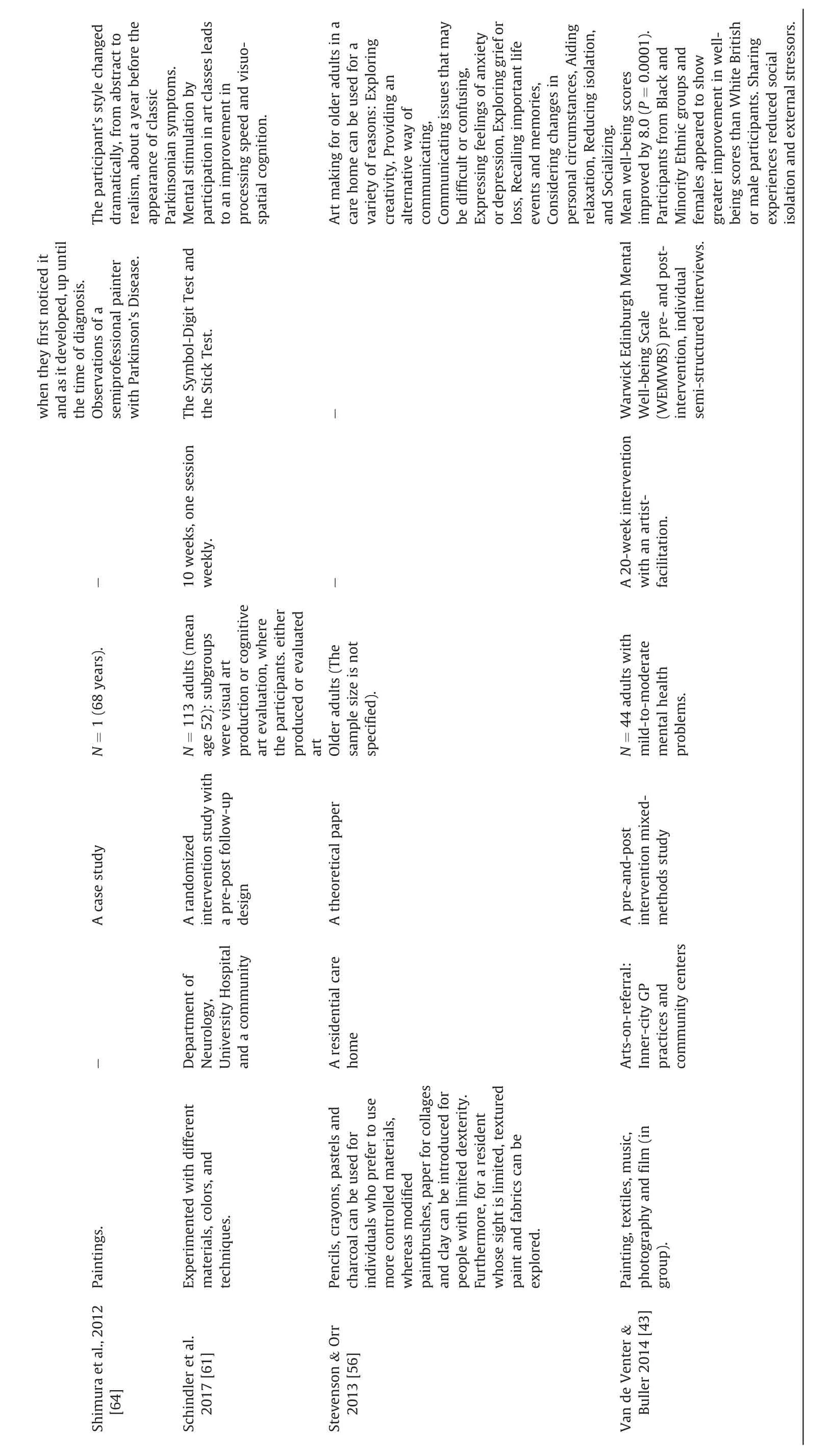
The data extracted from each paper (n=42) included:type of art making or expressive art therapy activity,context,research details(sample size and characteristics,intervention,method(s)of data collection) and outcomes and/or conclusions (theoretical papers).Following data charting and extraction,the data were summarized to answer the research questions [35,37].
5.Results
5.1.Art making in health and nursing care
Art making was described in 27 papers (Table 1),in contexts ranging from primary health care for community members[38-45]to a penal institution[46].The professional responsible for the art making was not always explicitly described,nor the involvement/role of researcher(s).Most participants were over 65 years of age.In seven papers,the art making activity was conducted in a group.In some papers,the persons involved in the art making could not speak [47,48].In one paper,patients’ near-ones were involved in art making[49]and in another paper,a member of the professional team made the art,emanating from the patient’s narrative [50].There were no papers in which health care or nursing professionals were solely engaged in art making.
The type of art making varied:drawing,painting,coloring,mosaic,sculpture,ballet,drama or furniture making (Table 1).In some papers,art making was considered a narrative(for example,[47,50-53]),while in other papers (for example,[39,46,49]) a narrative was produced as a complement to art making.In most papers,participants themselves chose the type of art making,but in some papers a pre-delineated art making scheme was seen.In some papers,the art making context and type of health problem were seen to influence the choice of art making materials [48,54-56].
Art making was described either as part of preventive health care on the individual level (for example,[42]) or group level (for example,38); or as a means for therapeutic nursing care.Art making was linked to the co-creation of new health indicators and community health [41],alleviating anxiety [38],and the improvement of emotional well-being[44,45],mental health[39,40,42]and personal growth [39,44].
In most papers,art making was described as a means for therapeutic nursing care,seen in various contexts and settings:specialized hospital mental care[43],pain care[57],oncologic care[58-60],neurologic care [61]rehabilitation [50,52,53],long-term elderly care (for example,[47,51,55,56,62]) and dementia care (for example,[48,49,63]).Art making was used as an assistive means in diagnosing Parkinson’s disease retroactively [64],a somatoformfunctional pain disorder [57]and melanoma [59].Within nursing care,art making activities were linked to outcomes(Table 2)such as acknowledgement of own unique experiences[52,56]or strengths[51],better communication of own experiences and strengths with professionals [50],heightened self-esteem [46,62],involvement in activity [53,55],less wandering for a person with dementia [48],and improvements in human connectivity[39]and social inclusion[49,56].Also,enhancement of own cognitive capacities [49,61],perceived lower anxiety [38],less physiologic stress [58],more positive emotions [60],improved mental well-being [43]and overall quality of life [49,50]were seen.
Information on art making activities in relation to preferred outcomes in the papers was dependent on research design and methodological rigor.Most papers were cross-sectional,did not include a control group,and had rather small sample sizes.The interventions,if described,were seen to vary in length from 20 min to 20 weeks and were not always fully described.Nevertheless,there were three randomized controlled studies and three longitudinal studies,and in most studies validated instruments were used during data collection,with or without qualitative methods.
5.2.Expressive art therapy in health and nursing care
Expressive art therapy was described in 15 papers (Table 3),in contexts ranging from community centers[65-68],projects for the homeless [69]and immigrants [68]to more clinical contexts:cancer care[70,71],dementia care[72,73],psychiatric care[74,75]and hospice care [76,77].Professional art therapists were responsible for the art therapy sessions,and researchers were seen to be involved data collectors.Most participants were elderly,usually over 70 years.In 11 papers,the expressive art therapy activities were organized in groups,despite the possible vulnerability of participants in certain contexts due to illness.In one paper,the person involved could not speak [72].There were no papers in which the patients’ near-ones or health and nursing care professionals were involved in expressive art therapy.
The type of expressive art therapy activity varied greatly:among others,music,guided imagery,coloring,sculpture,famous painting appreciation,quilting (Table 3).In all papers,the various activities were combined in accordance with how expressive art therapy was defined.For example,in some papers,narratives were considered an implicit part of the expressive art therapy process[65,68,69,73,74]while in other papers a narrative was produced as a complement to art making.In some papers,participants could choose between art therapy activities according to own preferences(for example,74) but in others a pre-delineated therapy program(for example,78) or art making scheme was seen.
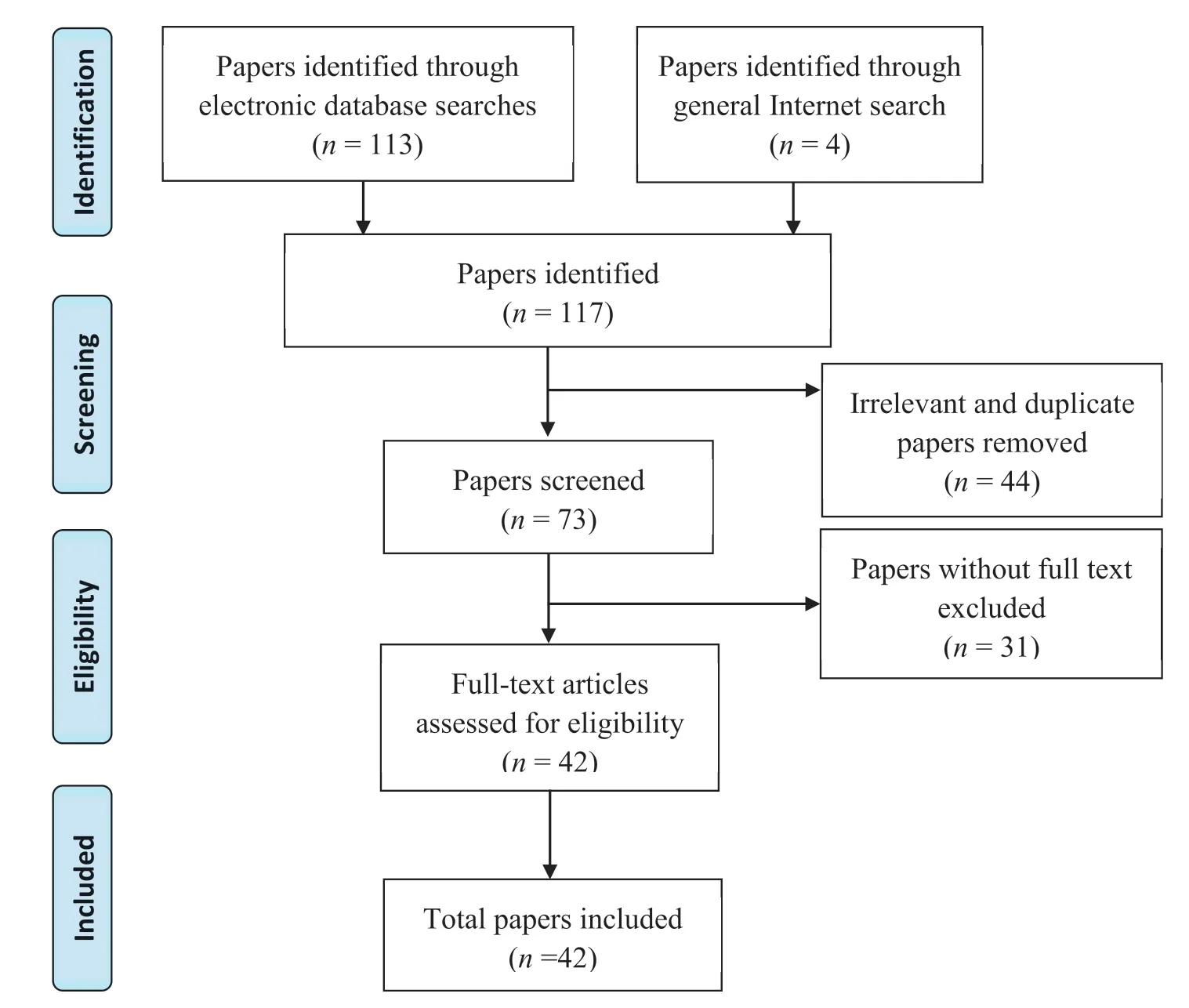
Fig.1.Flow diagram of paper selection process.
Expressive art therapy activities were linked to outcomes(Table 4) such as improved cognitive skills [65,66,68],self-esteem[74,78],connection with others such as family members and staff[67,77,78],self-expression [73,77,78],self-empowerment [76],quality of life [71,72,77],and self-efficacy [69],and decrease in depression[70,74,75,79],anxiety[70,75,78]and psychosocial stress[71].
Information on expressive art therapy activities in relation to preferred outcomes in the papers was dependent on research design and methodological rigor.There were five randomized controlled studies and one controlled intervention study,but also three case illustrations and some project descriptions.The interventions were seen to vary in length from one session to 20 weeks,and the sample sizes were small.In about half of the papers,validated instruments were used during data collection.However,there were also several papers in which observations or field notes were used as the main data collection method,and these did not include systematic explanations of how the data were analyzed.
5.3.Outcomes of art making or expressive art therapy activities in health and nursing care
While the outcomes linked to art making and expressive art therapy activities in adult health and nursing care are briefly described in sections 5.1 and 5.2 above,a synthesis of the stated relationships between the different types of activities and outcomes also occurred.The activities are listed in order from passive to more active engagement (Tables 2 and 4).
Little difference was seen between the activities included in art making and expressive art therapy activities.With few exceptions,such as singing,crafting,making videos and drama (art making)and guided imagery and viewing of artworks (expressive art therapy),all other activities were the same.
The outcomes of art making activities (Table 2) for individuals were linked to,for example,acknowledgement of own unique experiences and own strengths,personal growth,emotional wellbeing,heightened self-esteem and better communication of own experiences and strengths with professionals.The outcomes of art making activities in group were linked to the development of cognitive capacities (possibly),mental well-being,social inclusion and quality of life.
As seen in 11 out of 15 papers,expressive art therapy activities primarily took place in groups.The outcomes of expressive art therapy activities in group (Table 4) were linked to a decrease in certain symptoms such as psychosocial stress,anxiety or depression;or improved self-esteem,self-expression,self-empowerment and connection with others.
Outcomes linked to art making appear to encompass prevention,while outcomes linked to expressive art therapy appear to encompass the care and cure of already existing signs of health problems.Nonetheless,very similar goals,methods and outcomes for both methods were seen.Therefore,it is not relevant to state any relationships between certain health problems and the specific outcomes of art activities.
6.Discussion and conclusions



The aim of this scoping review was to describe the existing knowledge on art making and expressive art therapy in adult health and nursing care.From the 42 studies and other papers included here,published between 2010 and 2020,one sees that both art making and expressive art therapy are used on the community level in preventive health care and rehabilitation,as well as in hospitals and other care institutions in specialized nursing care and cure.In other words,the art activities were offered for both healthy individuals as part of community projects and for chronically or terminally ill residents,with activities for such participants occurring outside of the home setting (see Ref.[10]) and no acute patients being seen (see Ref.[2]).While this is understandable,because of the perceived challenges associated with organizing art activities in a home setting and the nature of acute health problems,art activities can nonetheless easily be organized in such a setting.Individuals can involve themselves in crafting or other art making activities in the home using independent virtual or digital devices.Researchers have shown that acute patients benefit from receptive art engagement in the form of paintings or music (see Ref.[4]),even if they are not willing or actively able to make art during an acute health problem.The art activities seen here were mainly organized as part of research or general projects,not as systematic health or nursing care interventions,even though most art activity types can be undertaken alone without any special skills and/or significant material investments.However,the context of art making and type of health problem influence the choice of art making type and materials[48,54-56].For example,patients with tendency to eat whatever they get into their hands (certain psychiatric conditions,deep dementia) or with risk to other kind of self-harm or aggression such as wounding cannot work with scissors or participate into crafting activities such as quilting,embroidery,needlework,leatherwork,woodwork,copper-tooling or metalcraft -at least not in group and without supervision.
Activation appeared to be one objective underlying the implementation of art activities.Usually organized in a group,art activities were seen to improve acknowledgement of own experiences,strengths and self-esteem; lead to better communication of own experiences and strengths with professionals; and improve perception of well-being or health on the psychological,physiological and social levels and quality of life.Another underlying objective appeared to the facilitation of the coping with and adapting to age-related transitions such as retirement,decrease of mobility,cognitive decline or move from own home to a nursing home.This was seen as support during an emotional crisis such as immigration,incarceration,homelessness or hospice care; facilitating coping with psychological and physical symptoms; or support during or after a health crisis such as depression,brain injury,cancer,chronic pain,open heart or hip replacement surgery.These results are in accordance with earlier research results (see Ref.[3,4,8,18]) and the definition of expressive art therapy (see Ref.[9]).Nursing goals and outcomes can be related to art activity outcomes,measured through observations of patients’art activities and narratives linked to such activities.
Art activities were linked not only to acknowledging and building new strengths and skills,making meaning of experiences,and personal growth but also the establishment of clinical diagnosis,symptom alleviation,and communication,whereby collaboration with near ones and health care professionals was fostered.Art activities should become an essential part of health and nursing care,because they were seen to be beneficial in nearly every context:prevention,rehabilitation,care,cure and palliation.They were furthermore seen to promote person-centeredness,whether organized for individuals or in group.
Health care professionals should be encouraged to use art activities intentionally to get to know each person and his/her experiences,because the meaning of the person’s experiences is a vital part of evidence-based nursing art and person-centered care(see 26,27,28,30).To achieve mutual understanding of both perceived symptoms,problems,needs,strengths and areas of satisfaction,nurses should encourage patients’ narratives and/or other creative expressions(see 3).Art making and/or expressive art therapy can also be used to address complex challenges (see 2),such as pandemics.For example,what are individuals,groups,nurses,patients,and near-ones experiencing during this most recent COVID19 pandemic? How could nursing education,health care organization and management be further developed,emanating from these experiences? In the data seen here,most participants were adults,aged 65 years or older.In most papers,even if the type of health problem has an impact on choice of safe art making materials,the participants themselves chose the preferred art activity,which is a motivating and truly personcentered act [2,15,22,31-33].Still,patients’ near-ones were involved in art making in only one paper[49],and a member of the professional team made art emanating from the patient’s narrative in only one paper[50].No papers describing collaborative patientprofessional art making or health care professional art making were seen (see 4,13).Also,the professional responsible for the art making was not always explicitly described,nor the involvement/role of researcher/s.
These results are partly contrary to recommendations on the use of art in health care.Engagement in art activities is linked to the engagement of patients’near-ones in person-centered care and the idea of sustainable methods whereby to promote the well-being of healthcare professionals; among other things,art activities have been shown to improve the mental health and well-being of personnel and reduce stress and burnout[4].There may be a lack of information about the importance of and possibility to include patients’ near-ones and health care professionals in art activities.Through more knowledge and understanding of the types and outcomes of art activities,health care personnel can inform patients,patients’near-ones and members of interprofessional teams about the importance of active art making and make what is seemingly currently“extraordinary”a more ordinary,implicit part of care.How health care personnel can facilitate art making should be included in health care professional curricula or offered as further education.In this data there was no evidence of such;neither in health care personnel education-nor patient education(see 12,20).
If health care personnel do not have time for art activities as part of their professional interventions,professional art therapists could be employed.However,if there is no need for professional therapy,the use of professional therapists can be considered an unnecessary barrier between the nurse and patient.Giving nurses the opportunity to incorporate art activities into their evidence-based,professional nursing interventions would promote an active nursing role and a creative,person-centered way of working.Moreover,a variety of artists,writing coaches or actors could be included not only in interprofessional health care and nursing teams but also in care for health care personnel,which could help facilitate sustainable creativity.
Further randomized controlled trials in which the use of art making or expressive art therapy are investigated in relation to their effects on the nurse-patient relationship,the patient-nearone relationship,person-centeredness,clinical and other outcomes are needed.This can help ensure that art activities and narratives emerging from such activities become an effective means for the realization of person-centered preventive health care,nursing care and cure,nursing education and sustainable care for health care personnel.Also,health care professionals’ knowledge of,skills and attitudes toward art activities should be investigated,alongside measurement of art activity outcomes over a longer period of time and broader samples,in which participant life situation,education,cognitive and motoric capacities are explored.Lastly,more male participants and participants from differentethnic backgrounds are needed.

Table 2 Outcomes of art making activities.

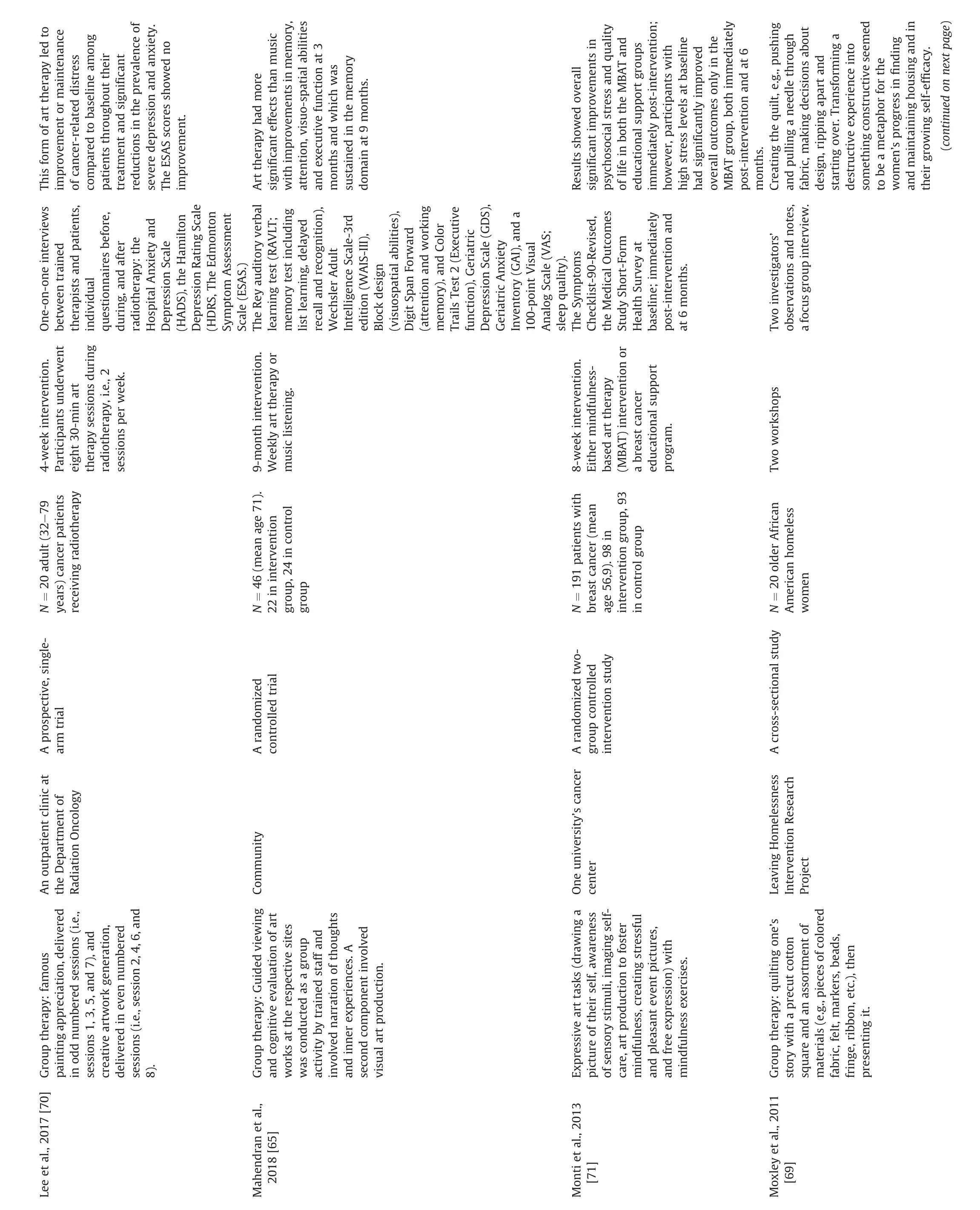

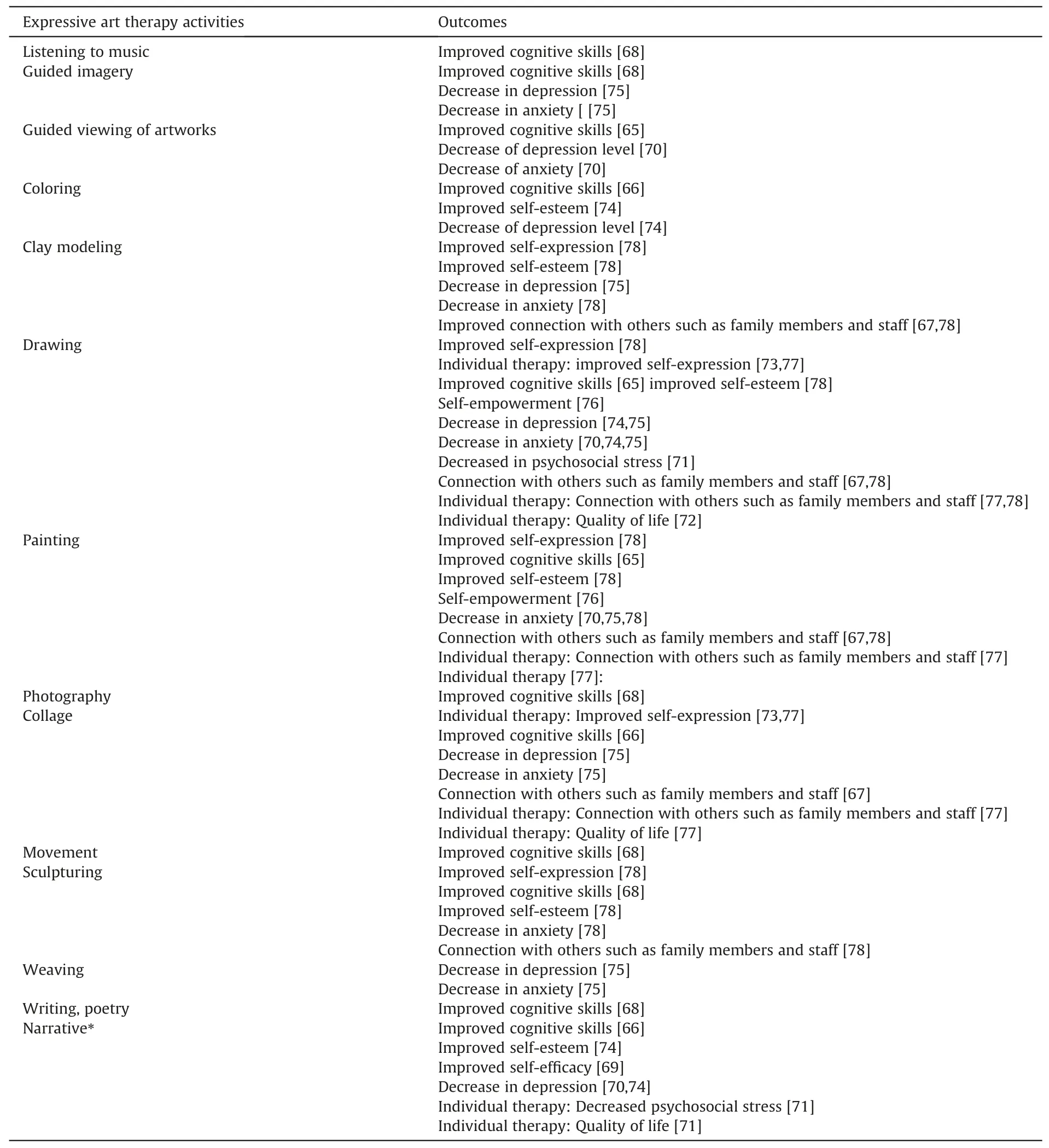
Table 4 Outcomes of expressive art therapy activities.
This review has some limitations.The data search was conducted by one author,and there is no registered review protocol,only manual documentation of the search process.The search yielded in 117 papers of which 31 were not available in full-text without economic investment.However,all the abstracts were read through properly by all authors and we are convinced that if we would have purchased those papers the main results of this scoping review would not have altered.The data charting and extraction were conducted by the entire research group.Some data in the papers reviewed were not always explicitly reported:the art making or expressive art therapy intervention,health care professionals’ and/or researchers’ role,the data analysis process.Also,sample sizes were smallish and the availability of follow-up data on the long-term effects of art activities was limited.
CRediT authorship contribution statement
Heli Vaartio-Rajalin:Conceptualization,Methodology,Data Curation,Visualization,Formal Analysis,Writing -Original Draft,Supervision.Regina Santam¨aki-Fischer:Conceptualization,Data Curation,Validation,Writing-Review&Editing.Pamela Jokisalo:Data Curation,Validation,Writing -Review & Editing.Lisbeth Fagerstr¨om:Validation,Writing -Review& Editing.
Funding
This research did not receive any specific grant from funding agencies in the public,commercial or not-for-profit sectors.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2020.09.011.
 International Journal of Nursing Sciences2021年1期
International Journal of Nursing Sciences2021年1期
- International Journal of Nursing Sciences的其它文章
- Focuses and trends of the studies on pediatric palliative care:A bibliometric analysis from 2004 to 2018
- Relationship between negative emotions and perceived support among parents of hospitalized,critically ill children
- The effect of digital health technologies on managing symptoms across pediatric cancer continuum:A systematic review
- Effectiveness of animal-assisted therapy on pain in children:A systematic review and meta-analysis
- Effects of creative expression program on the event-related potential and task reaction time of elderly with mild cognitive impairment
- Struggling to live a new normal life among Chinese women after losing an only child:A qualitative study