
Laparoscopic treatment of pyogenic liver abscess caused by fishbone puncture through the stomach wall and into the liver: A case report
2023-01-04 07:59AbudureyimuKadiTalaitiTuerganYierpanAbulaitiPaizulaShalayiadangBaihetiyaerTayierAbududuainiAbuliziMuniremuTuohutiAyifuhanAhan
World Journal of Clinical Cases 2022年36期
Abudureyimu Kadi, Talaiti Tuergan, Yierpan Abulaiti, Paizula Shalayiadang, Baihetiyaer Tayier, Abududuaini Abulizi, Muniremu Tuohuti, Ayifuhan Ahan
Abudureyimu Kadi, Talaiti Tuergan, Yierpan Abulaiti, Paizula Shalayiadang, Baihetiyaer Tayier,Abududuaini Abulizi, Ayifuhan Ahan, Department of Hepatobiliary and Hydatid Disease,Digestive and Vascular Center, First Affiliated Hospital of Xinjiang Medical University,Urumqi 830054, Xinjiang Uygur Autonomous Region, China
Muniremu Tuohuti, Department of General Medicine, First People's Hospital of Aksu Region,Aksu 843099, Xinjiang Uygur Autonomous Region, China
Abstract BACKGROUND Pyogenic liver abscess (PLA) due to foreign body penetration of the gastrointestinal tract is rare but can lead to serious consequences if not diagnosed and managed properly. We report a case of PLA caused by a fishbone puncture.CASE SUMMARY This report describes the clinical features, diagnosis and treatment of a 56-yearold male patient who presented with severe pneumonia, acute respiratory failure and septic shock. The main clinical manifestation was a nonspecific recurrent infection. Based on the findings of abdominal computed tomography examination and the detailed medical history, the diagnosis was made as PLA which was caused by fishbone puncture through the stomach wall and into the liver. After active anti-inflammatory treatment, the patient's general condition had improved. The laparoscopic drainage of the liver abscess and the foreign body removal was performed. There was no recurrence of abscess at discharge or during follow-up and the patient’s general condition was satisfactory.CONCLUSION PLA caused by foreign bodies usually requires surgical treatment or percutaneous drainage combined with antibiotics. Our case confirms that a laparoscopic approach is safe and feasible for such cases.
Key Words: Liver abscess; Fish bone; Foreign body; Laparoscopic surgery; Case report
INTRODUCTION
Although ingestion of foreign bodies is common, complications are relatively rare in the clinical setting. Pyogenic liver abscess (PLA) due to gastrointestinal perforation by foreign bodies is even rarer, and the diagnosis is challenging due to the nonspecific symptoms and imaging difficulties. Timely diagnosis is very important for improving patient prognosis. If not timely diagnosed, surgical intervention for such cases may not be conducted in time, which may lead to serious consequences. This report presented a case with PLA caused by a fishbone puncture through the stomach wall and into the liver. The clinical features, diagnosis and treatment of this case were described. The report would contribute to the timely and accurate diagnosis and the treatment of PLA caused by foreign bodies.
CASE PRESENTATION
Chief complaints
A 56-year-old male patient presented with complaints of intermittent chest tightness and shortness of breath for 7 d, worsening for 1 d, and was admitted to the intensive care unit of the Emergency Department.
History of present illness
The patient presented with chest tightness and shortness of breath about 1 wk ago. One day prior, the aforementioned symptoms progressed and the patient further developed tremor of the hands, loss of appetite, general malaise and loss of consciousness without obvious cause.
History of past illness
The patient had no history of alcohol consumption, drug abuse or other high-risk behaviors causing PLA. He was in good health and denied any history of hypertension, diabetes and/or heart diseases.
Personal and family history
The patient denied any family history of hypertension, diabetes and heart diseases.
Physical examination
The patient’s abdomen was soft with right upper quadrant tenderness but there was no rebound pain or muscle tension. The vital signs were as follows: Body temperature 39.2 °C; blood pressure 98/56 mmHg; heart rate 84 beats per min; respiratory rate 26 breaths per min. There was no obvious abnormalities in other physical examinations.
Laboratory examinations
Laboratory examinations showed that the white blood cell count was 22.22×109/L; neutrophil percentage was 91.7%; platelet count was 26 × 109/L; pH was 7.28; PCO2was 27 mmHg; PO2was 64 mmHg; HCO3-was 12.7 mmol/L; BE (Base Excess) was -12.5 mmol/L; C-reactive protein level was > 90 mg/L; interleukin 6 was > 5000 pg/mL; procalcitonin was > 100 ng/mL; and, myoglobin was > 2000 ug/L.
Imaging examinations
The cranial computed tomography (CT) showed that the soft tissue of the posterior top of the nasopharynx was slightly thicker. The thoracic CT observed that there were bilateral pneumonia, lung air sac in the right lung apex, multiple nodules in bilateral lungs and bilateral pleural effusion. On the abdominal and pelvic CT, there were foci with a slightly lower density in the right lobe of the liver and mixed density in segment IV of the liver near the first porta hepatis.
MULTIDISCIPLINARY EXPERT CONSULTATION
Multidisciplinary team (MDT) discussion results were as follows: On abdominal CT, there was a needlelike high-density shadow in the liver, however, this was missed in the initial report (Figure 1). The drainage from the indwelling gastric tube was brown, which suggests purulent infection. Based on these findings, we presumed that the cause of the PLA may be that the accidentally ingested fishbone may have pierced the pylorus and penetrated the liver, causing local inflammatory reaction, abscess, and the corresponding clinical manifestations. After reviewing the medical history again, it was found that the patient did have a history of eating fish a few days before the onset of disease
FINAL DIAGNOSIS
The final diagnosis was PLA caused by fishbone puncture complicated with severe pneumonia, acute respiratory failure, and septic shock.
TREATMENT
The patient received anti-inflammatory rescue therapy, electrolyte correction, and nutritional support for 8 d in the intensive care unit, and then was transferred back to the general ward. However, the patient had recurrent fever without significant decreases in the inflammatory index and was returned to the intensive care unit again. Repeat abdominal CT showed combined density, and PLA was considered based on the medical history. The diagnosis and cause of PLA were discussed by MDT. Subsequently, the patient was transferred to the Hepatobiliary Surgery Department for laparoscopic exploration. A multiport laparoscope was used. An inspection hole was made above the navel in order to introduce the laparoscope and the remaining three trocars. During the operation, it was found that there were dense adhesions between the pylorus and hepatic hilum and the liver was obviously swollen at the root of the ligamentum teres. After incision, a white foreign body about 2 cm long was found (Figure 2A), which was confirmed to be a fishbone after removal (Figure 2B). An abscess cavity was found by further indeep exploration, which was incised and the white pus was drained. The abscess cavity was expanded and a drainage tube was placed for adequate drainage.
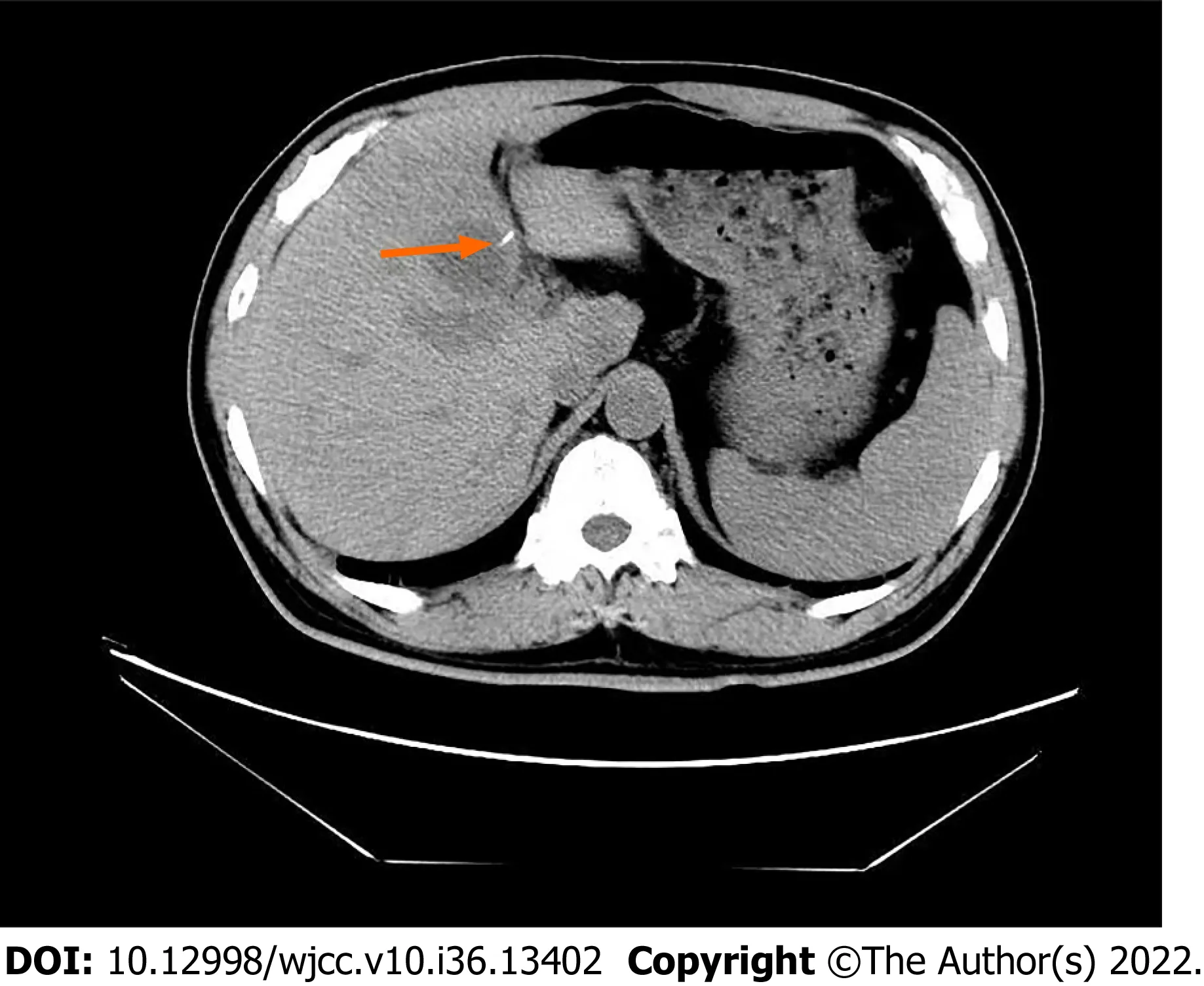
Figure 1 Computed tomography scan showing a foreign body in the left lateral segment of the liver. The high-density foreign body is marked with an orange arrow.

Figure 2 Intraoperative findings. A: It was observed that a fishbone penetrated the liver and formed a purulent cavity; B: Removal of fishbone by laparoscopic surgery.
OUTCOME AND FOLLOW-UP
After the operation, the patient recovered smoothly. A small amount of reddish drainage fluid was observed. After 5 d of observation, the inflammatory indexes were decreased, and the above symptoms and discomfort disappeared. The drainage tube was therefore removed. The patient was discharged in stable condition. Follow-up at 2 wk and 2 mo after discharge was unremarkable.
DISCUSSION
Liver abscesses are purulent lesions of the liver caused by various pathogens such as bacteria, fungi or Entamoeba histolytica. Biliary route, portal vein route, hepatic artery route, cryptogenic route and direct route to the liver from an open wound are the common infection routes of bacterial liver abscess. Hepatic artery and open wound routes are relatively rare in clinical practice, but cannot be ignored[1]. PLA caused by foreign bodies are rare[2]. It has been reported that the incidence of foreign body penetration of the gastrointestinal tract is less than 1%, and the most common sites of gastrointestinal perforation include the stomach and duodenum. Accidental ingestion of foreign bodies is not uncommon, and the vast majority (80%-90%) of the ingested foreign bodies pass naturally through the gastrointestinal tract within 1 wk. In fact, less than 1% of the patients who ingest foreign bodies could experience symptoms, which are usually secondary to gastrointestinal obstruction or perforation[3]. PLA secondary to foreign body penetration of the gastrointestinal tract are even more rare. Lambert[4] reported the first case in 1898. Since then, there has been an increasing number of studies on such cases, especially over the past 40 years. The duodenum and pylorus may be more prone to perforation[5].PLA caused by perforation of fishbone through the stomach is relatively hidden and dangerous, which can often bring serious consequences. Theodoropoulouet al[6] reported a high fever in a 46-year-old man without comorbidities, who died of sepsis within 46 h of admission. In the autopsy, a fishbone was found in the liver. Their report points to the level of vigilance clinicians must be aware of in each particular case and this clinical presentation is very similar to our case reported herein. PLA is a disease well known to clinicians and its clinical manifestations are diverse. Some patients present with high fever, right upper quadrant pain, and jaundice. Most patients would be cured after anti-infective treatment, puncture, and drainage. More dangerous and systemic infection with PLA requires the identification of the cause, especially if the patient has no major infectious factors such as biliary tract infection, blood infection or diabetes. In this report, the thickening of the gastrointestinal tract adjacent to the abscess on the preoperative CT examination, as well as the presence of intraoperative adhesions, were clues of PLA secondary to foreign body penetration of the gastrointestinal tract. The clinical manifestations of PLA caused by foreign bodies are usually ambiguous and nonspecific, but abdominal pain (77.3%) and fever (58%) are the most common symptoms[7,8]. Occasionally, acute upper gastrointestinal bleeding may be present[9]. Chenet al[10] have summarized 86 cases of liver abscess caused by foreign bodies such as toothpicks, fishbones, chicken bones, needles,etc.They listed many groups at risk for foreign body perforations, including prison inmates, mentally ill, alcoholics, children, the elderly, carpenters, and tailors. Other conditions included fast food, hot or cold drinks, cognitive impairment, and people wearing dentures. Early identification and extraction of foreign bodies causing gastrointestinal perforation is critical to avoid morbidity and mortality[11,12]. However, early diagnosis is challenging due to the lack of specific findings, the lack of patient awareness of foreign body ingestion, and the low index of suspicion by the medical team for the specific condition. Liver abscess due to foreign body ingestion is still rare and a difficult diagnosis because most patients do not recall foreign body ingestion events and usually present with nonspecific symptoms[13]. Moreover, the foreign bodies are not visible on X-rays and sometimes not even on CT scans.
It is worth noting that there can be a considerable time span of months or even years between the ingestion event and the onset of symptoms of an inflammatory lump or abscess. If foreign body perforation is not properly diagnosed in a timely manner, percutaneous interventional drainage can lead to recurrence or persistence of abscesses, and can even lead to a life-threatening sepsis. Therefore, in refractory abscess after interventional drainage and antibiotics, PLA caused by foreign bodies, although rare, should be considered as the underlying pathogenesis. Clinicians should also be aware that older adults wearing dental prosthetic devices may ingest foreign bodies. CT scans are currently the gold standard for diagnosing foreign body ingestion due to their high resolution and accuracy. Foreign bodies usually appear as high-density linear objects on CT, and CT scans of foreign body ingestion can also determine the presence of perforation, the degree of intra-abdominal inflammation with or without abscess formation, and adjacent organ damage[14]. Contrast-enhanced CT scan is the standard diagnostic modality that provides high resolution and accuracy, followed by abdominal ultrasound[15]. In this report, CT scan was also used for diagnosis. For patients with poor tolerance, unstable vital signs, or contraindications to resection, conservative treatment and supportive treatment can be accepted as the first step, and the situation will improve after re-evaluation. The removal of foreign bodies can be considered at the time of diagnosis. In the 86 cases summarized by Chenet al[10], the foreign bodies in the liver were successfully removed after exploratory laparotomy and 2 cases received laparoscopy for foreign body removal. Comparing the difference between traditional exploratory laparotomy and laparoscopy, it could be concluded that the postoperative hospital stay after laparoscopic surgery is significantly shorter than that of laparotomy. Burkholder and Samant[16] treated a case with fish boneinduced liver abscess with antibiotics and percutaneous drainage, avoiding the need for open surgical intervention. They concluded that percutaneous drainage was the appropriate first line treatment in most cases, even in cases of retained foreign body. When the percutaneous drainage and antibiotics are not effective, removal of foreign bodies causing the PLA is necessary, and laparoscopic surgery is an effective method for the treatment of PLA caused by foreign bodies[17].
CONCLUSION
Cases of PLA secondary to foreign body penetration of the gastrointestinal tract are extremely rare, the diagnosis of which requires comprehensive analysis and evaluation of the medical history, imaging data, disease progression and systemic condition. Surgery is an effective way to remove the cause, and laparoscopic removal of the foreign bodies is also an effective minimally invasive treatment. Meanwhile, clinicians should improve the understanding of this type of disease, and achieve early detection and early treatment, which is conducive to the prognosis of patients.
FOOTNOTES
Author contributions:Kadi A and Tuergan T are the co-first authors who organized the case content, collected all relevant data and drafted the manuscript; Shalayiadang P performed the surgical procedure; Tayier B and Tuohuti M participated in collecting the clinical data; Abulaiti Y and Abulizi A performed the literature research and contributed to manuscript revision; Ahan A conceived the study design, interpreted all data and revised the manuscript in depth; all authors have read and approved the final manuscript.
Supported bythe Open Project of the State Key Laboratory of Pathogenesis, No. SKL-HIDCA-2019; and Prevention and Treatment of High Incidence Diseases in Central Asia jointly established by the Provincial Government and the Ministry, No. SKL-HIDCA-2022-34.
Informed consent statement:Informed written consent was obtained from the patient for publication of this report and any accompanying images.
Conflict-of-interest statement:All the authors report having no relevant conflicts of interest for this article.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016), and the manuscript was prepared and revised according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers. It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BYNC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is noncommercial. See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:China
ORCID number:Abudureyimu Kadi 0000-0002-8376-5417; Talaiti Tuergan 0000-0002-3833 -7253; Yierpan Abulaiti 0000-0001-6187-7015; Paizula Shalayiadang 0000-0003-4869-9351; Baihetiyaer Tayier 0000-0002-4828-7827; Abududuaini Abulizi 0000-0003-0700-8630; Muniremu Tuohut 0000-0001-7004-2183; Ayifuhan Ahan 0000-0002-5751-821X.
S-Editor:Xing YX
L-Editor:Filipodia
P-Editor:Xing YX
 World Journal of Clinical Cases2022年36期
World Journal of Clinical Cases2022年36期
- World Journal of Clinical Cases的其它文章
- Liver injury in COVID-19: Holds ferritinophagy-mediated ferroptosis accountable
- Amebic liver abscess by Entamoeba histolytica
- Living with liver disease in the era of COVID-19-the impact of the epidemic and the threat to high-risk populations
- Cortical bone trajectory screws in the treatment of lumbar degenerative disc disease in patients with osteoporosis
- Probiotics for preventing gestational diabetes in overweight or obese pregnant women: A review
- Effectiveness of microwave endometrial ablation combined with hysteroscopic transcervical resection in treating submucous uterine myomas