
Strengths,weaknesses,opportunities and threats of peer support among disadvantaged groups: A rapid scoping review
2023-11-26 05:22KlinMikoljczkDegruweSyrenSlimmenDylnGillissenPetrdeBilVlerieBosmnsCorrineKeeminkIngeMeyvisYvonneKuipers
Klin Mikoljczk-Degruwe ,Syren R.Slimmen ,Dyln Gillissen ,Petr de Bil ,Vlerie Bosmns ,Corrine Keemink ,Inge Meyvis ,Yvonne J.Kuipers ,c,*
a Research Group Healthy Region, HZ University of Applied Sciences, Vlissingen, Netherlands
b Department of Health and Social Studies, School of Midwifery, Artesis Plantijn University of Applied Sciences, Antwerp, Belgium
c School of Health and Social Care, Edinburgh Napier University, Edinburgh, UK
Keywords:Peer support Scoping review Sociological factors Vulnerable populations
ABSTRACT Objective: To explore the current state of knowledge and evidence about peer support for various disadvantaged groups;to identify the strengths,weaknesses,opportunities,and threats of peer support to critically reflect on peer support within health and social services.Methods: A rapid scoping review was conducted according to Arksey and O’Malley’s framework,aiming to identify eligible studies in PubMed,APA PsychInfo,Education Resources Information Center,Cochrane Library,Academic Search Premier,ScienceDirect,Directory of Open Access Journals,ResearchGate,WorldCat,and Google Scholar.According to Rodgers’ concept analysis steps and the SWOT model,data was reported using thematic synthesis.Results: Forty-five studies were included,describing a variety of peer support initiatives among groups of young migrants and unsupervised minors,young adults with autism,people with (mental) health problems,foster/shelter families,vulnerable pregnant women,people outside the labour force,older adults,and homeless people.The strength of peer support is its positive effect on the quality of life among vulnerable people.The weakness is represented by peers both being too involved and focused on personal interest or by peers lacking expertise and knowledge.Opportunities for peer support are mutual learning,the anticipated long-term effects,and the potential to facilitate social inclusion.Culture,language barriers,drop-out rates,securing sustainability,and peers’ lack of time and commitment are regarded as threats to peer support.Conclusion: Although peer support offers good outcomes for various groups of vulnerable people,the weaknesses and threats need to be considered to provide and proliferate peer support.
What is known?
· Peer support involves people drawing on shared personal experiences or characteristics to help one another.
· We need to make better use of community resources.
What is new?
· The study provides an overview of various target groups and the extent to which peer support is received or offered,highlighting the key elements of peer support.
1.Introduction
Worldwide,individuals and groups face barriers to access and participate in social life.A growing number of socially disadvantaged people whose needs are not recognised or met by current health and social care structures and services are more likely to become vulnerable [1,2].Vulnerability can relate to gender,age,race,ethnicity,religion,citizenship status,disability,and occupation -aspects that label and stigmatise individuals and groups [3].During times of need and distress,individuals turn to social relationships for support,often in response to barriers or deficiencies encountered in the present health and social care system.In recognition of the importance of social relationships,peer support has been recognised as a solution to reach socially vulnerable people to prevent catastrophe and excesses,to improve equity and individuals’ connection to the community,to facilitate psychosocial adjustment (emotional,healthy behaviour and disease management) and to support and to empower individuals[4-7].
Peer support is a powerful method in human behaviour and health and social inclusion [4,6,7],receiving a strong emphasis in the WHO’s Global Health Workforce Alliance [8].The concept of peer support in health and social care has been defined as: “the provision of emotional,appraisal,and informational assistance by a created social network member who possesses experiential knowledge of a specific behaviour or stressor and similar characteristics as the target population,to address a health-related issue of a potentially or stressed focal person” [5].Peer support is nonhierarchal and is provided by peer lay individuals or paraprofessionals with experiential knowledge who connect individuals and services,extend natural(embedded)social networks,and complement professional health services [5].Economic analyses of peer support initiatives have shown economic benefits[9].
Peer support,however,is complex,inconsistent,and diverse in its application [4-7].It is unknown if the positive effect of peer support is achieved by the ‘sum of its parts’ or whether there are distinct features that contribute to its impact.In response to the known benefits of peer support,its diversity,and the unknown overall effect or the effect of its different elements,it is of merit to comprehensively explore the extent to which peer support can be used to pertain to and increase its implementation.This paper aims to explore and gain insight into the current knowledge and evidence about peer support.It provides a better understanding of using the method,its strategies,and how it might complement professional health and social services.Ultimately,to narrow the gap between excluded and vulnerable individuals and groups and services -facilitating social inclusion.
This paper was written as part of the ENSURE Interreg 2Seas Mers Zee¨en project (https://www.interreg2seas.eu/nl/ENSURE).This project aimed to provide inclusive peer-support and to enable positive community development.The outputs of the project will consist of 1) developing a model linking peer-to-peer community volunteers/supporters,professionals,and vulnerable groups in society -the latter labelled by the characteristic that pre-determine them as being vulnerable,and 2)developing a training program for health,social care &welfare professionals/volunteers/nongovernmental organisations (NGO),based around mentalization and for peer-to-peer community volunteering acting as intermediaries between vulnerable individuals and state services.The outputs will have an inclusive and co-creative character,aiming to suit all groups in the community,drawing upon what works and on the current gaps that need to be addressed.
The ENSURE project group contains several social and healthcare partners and NGO’s from the four European coastal North Sea Channel areas (France,Belgium,Netherlands,and the United Kingdom).The project group is diverse in structure,including parties that target a variety of groups,such as (young) migrants,refugees,and status holders,people with an ethnic background different from the country of habituation,young adults with autism,care avoiders,people on welfare,non-accompanied minors,foster children and foster families,isolated individuals,pregnant women,unemployed/unskilled/untrained people.All project partners developed some form of peer support within their services based on expertise and progressive insights as a result of involvement with their target groups-with varying effects,outcomes,and success.ENSURE parties would benefit from evidence that indicates strengths,weaknesses,opportunities,and threats of peer support to inform the development of the ENSURE project’s model and the training programs.Therefore,to inform and optimise the application of peer support to benefit a wider service provision,seeking evidence comprehensively and systematically on how and to which extent peer support is offered is needed.This paper is the first step of the ENSURE project to inform the further development of the outputs.
2.Methods
A rapid scoping review,an approach used to cover a vast volume of literature on a broad topic,was considered the best method for producing a broad overview of the area of interest [10-13].Opposed to a systematic review,a rapid review allows to synthesise evidence without delays,is timely and resource-efficient to inform target audiences such as policymakers,health,social care,and welfare organisations,and NGO’s -like the ENSURE project partners -to direct transformation and to provide information for strategic focus [13-15].The approach described in the WHO’s practical guide for rapid reviews[14],directed the method for this study.The current rapid scoping review protocol was structured using the scoping review methodological framework described by Arksey and O’Malley[11].
2.1.Search strategy
An extensive literature search was conducted to identify studies published from the earliest date in each database until March 2020.The timetable of the project determined the end date of the search;the review served to inform the next step of the project.It was anticipated that searches would result in a broad range of studies.To narrow this down,the search was designed to retrieve all texts covering multiple target groups’ vulnerability concepts.Search terms were therefore formulated in agreement with the ENSURE project partners,and target groups were chosen based on the character of the project partners’ service users.One author performed a search per population/target group,which is common in a rapid review [13].A mixture of keywords was used to guide searches joined together by the Boolean operators (AND,OR):((((((peer support OR peer-to-peer OR peer-led OR peer group)AND(inclusion) AND (social skills OR social participation OR interpersonal relation) AND (support OR caregiver OR informal care OR nonrelative OR family OR parent) AND (community) AND (target group))))).A search term representing the specific target group was imputed,such as young migrants and refugees (migrants OR refugees OR asylum AND young OR minors OR adolescent OR unsupervised),young adults with autism(autistic OR autism OR autistic spectrum disorder AND young OR adolescent OR child),individuals with (mental) health issues (mental OR psychiatric OR disease),foster families (foster OR shelter),older adults (elderly OR older adults OR senior),pregnant women (pregnant OR pregnancy AND vulnerable),people outside the labour force (unemployed OR unskilled OR untrained AND poverty OR low income OR financially disadvantage OR homeless).The main search strategy was systematically applied to the following electronic collections,databases,and academic search engines: PubMed,APA PsychInfo,Education Resources Information Center (ERIC),Cochrane Library,Academic Search Premier,ScienceDirect,Directory of Open Access Journals,ResearchGate,WorldCat,and Google Scholar.These sources were considered most suitable and relevant for the topic of study [14].
Several criteria were applied to the searches.Studies published in peer-reviewed journals,books,book chapters,guidelines,and conference papers available in English and studies with participants of all ethnicities performed in any country were considered eligible.Studies with a quantitative,qualitative,or mixed-methods study design were suitable.Studies referring to the specified target populations,part of the ENSURE project group (i.e.[young] migrants,young adults with autism,people on welfare,nonaccompanied minors,foster/shelter families and children,pregnant women with specific psychosocial needs,care avoiders,physically and emotionally neglected people,people with[mental]health issues,and homeless people) were included.Studies that referred to peer support (of any form) as an intervention were included.Studies that compared peer support with other forms of support provided by lay individuals or paraprofessionals (e.g.,buddy support,group support,student support,neighborhood support) were included.
2.2.Screening and charting
Per target group,the screening and charting were independently performed by one reviewer [13,14].The titles and abstracts of books,book chapters,guidelines,and conference papers and articles were screened according to the described criteria.The full texts were assessed for final inclusion.
2.3.Literature analysis
To systematically analyse how peer support is unambiguously used in various disciplines and services,Rodgers’ concept analysis steps were chosen to guide the process of exploring,extracting,and describing the antecedents,attributes,and consequences of peer support within each target group and record [16].The text of the records served as the data source.Per the target group,two authors(CK&YK,IM&VB,KM&PdB,SS&DG)charted the data in an MS Excel spreadsheet© to categorise the relevant information comprehensively and accurately.This way,each target group’s concept of peer support was described.All authors combined,compared and discussed the charts to create a multidisciplinary perspective to detect similarities and differences of antecedents,attributes,and consequences of peer support [17].
A second analysis was performed using the SWOT model -a simple but effective framework for analysing and synthesizing data and information to identify and maximise strengths,overcome or minimise weaknesses,exploit opportunities,and identify threats of intervention,project,or situation [18].Per target group,two authors extracted the strengths,weaknesses,opportunities,and threats of peer support,drawing on thematic synthesis.The MS Excel spreadsheets© served as the data source.As a next step,all authors compared and discussed the results,reaching a consensus about peer support’s general strengths,weaknesses,opportunities,and threats.All authors agreed with the final content.Considering the nature and the purpose of the review,no critical appraisal of the content of the studies included was required for selection[11,13,14].
3.Results
3.1.Literature search results
A total of 1,224 records identified via the databases were screened for title and abstract,of which 140 records were selected for full-text review.After reading the full texts,45 records were included (Fig.1).The papers and books were published between 1989 and 2020.The included studies were undertaken in the following countries: former Yugoslavia [19],Belgium [20],Netherlands [21,22],Australia [23,24],Canada [25-29],United Kingdom (UK) [26,30-33],United States (USA) [34-52,60],Italy[53],China [54],South Africa [55],Ireland [26,56],and Germany[57-59].Some reviews did not clearly specify the countries of the included studies [26,27,39,41,50,61-63].
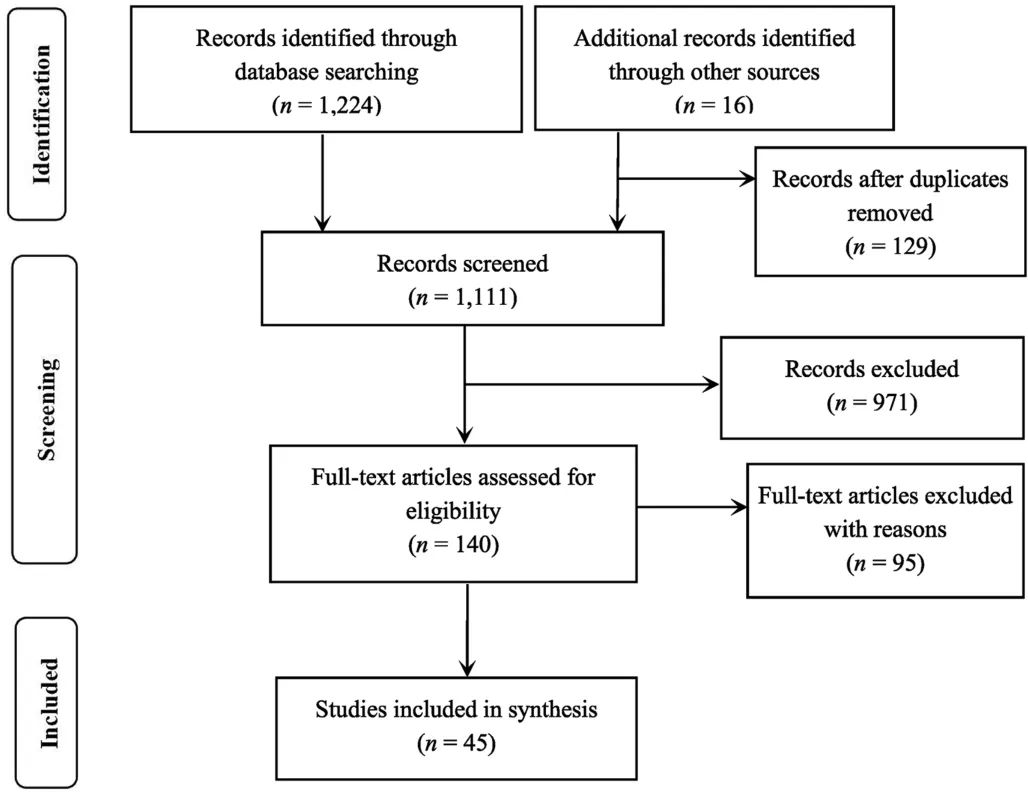
Fig.1.Flowchart of the study selection process.
3.2.Methods reviewed studies
The 45 records included 12 randomised (controlled) trials[24,25,30,38,40,42,43,45,47,56,59],one discussion paper [27],six reviews [39,41,50,60-62],one meta-analysis [63],one narrative review [26],four pilot studies [23,37,58],14 surveys[19,22,25,29,34-37,46,48,51,52,55,58],one case study [21],and 18 qualitative studies,using diaries [22],focus groups [33,44,46],observation [21],and interviews [19-21,28,31,32,46,49,54-59].
3.3.Content and nature of the peer interventions
The peer interventions varied in nature,strategies,and content:cognitive-behavioural group-based support [19,51],communal living [20],social networking [34,38,39,41,44,62],mentoring[23,39,56],(daily) in-person,telephone and online social media interaction [21,22,25,28,29,33,35,39,56,57,60,61],support (in coping) [20,30,52],home visits [49,50,55,56,63],counselling[29,31,32,36,48,58],story-sharing/narrating [52,61],coaching [41],training [34,41,42],education/knowledge and information sharing[27,33,35,37,38,43,44,54,57,59,60,63],recreational activities[29,35,49],companionship/befriending [30,47,49],modelling[24,45,61],roleplay [40,45],goal setting [37,41,43],financial assistance [39,41],and practical support [29-31,37,49,57].
3.4.Type of peers
The type of buddies[22],students[23,33,36],parents[27,28,50],administrators [48],family members [50-52,54],informal caregivers [40,42,46],volunteers [26,29,41,63],volunteers with similar lived experiences/experiential knowledge [25,30-32,37],locals[20,26,30,49],and (semi)professionals[33,41,44,45,48,51,52,57-59,63].The characteristics of the 45 included records are presented in Table 1.
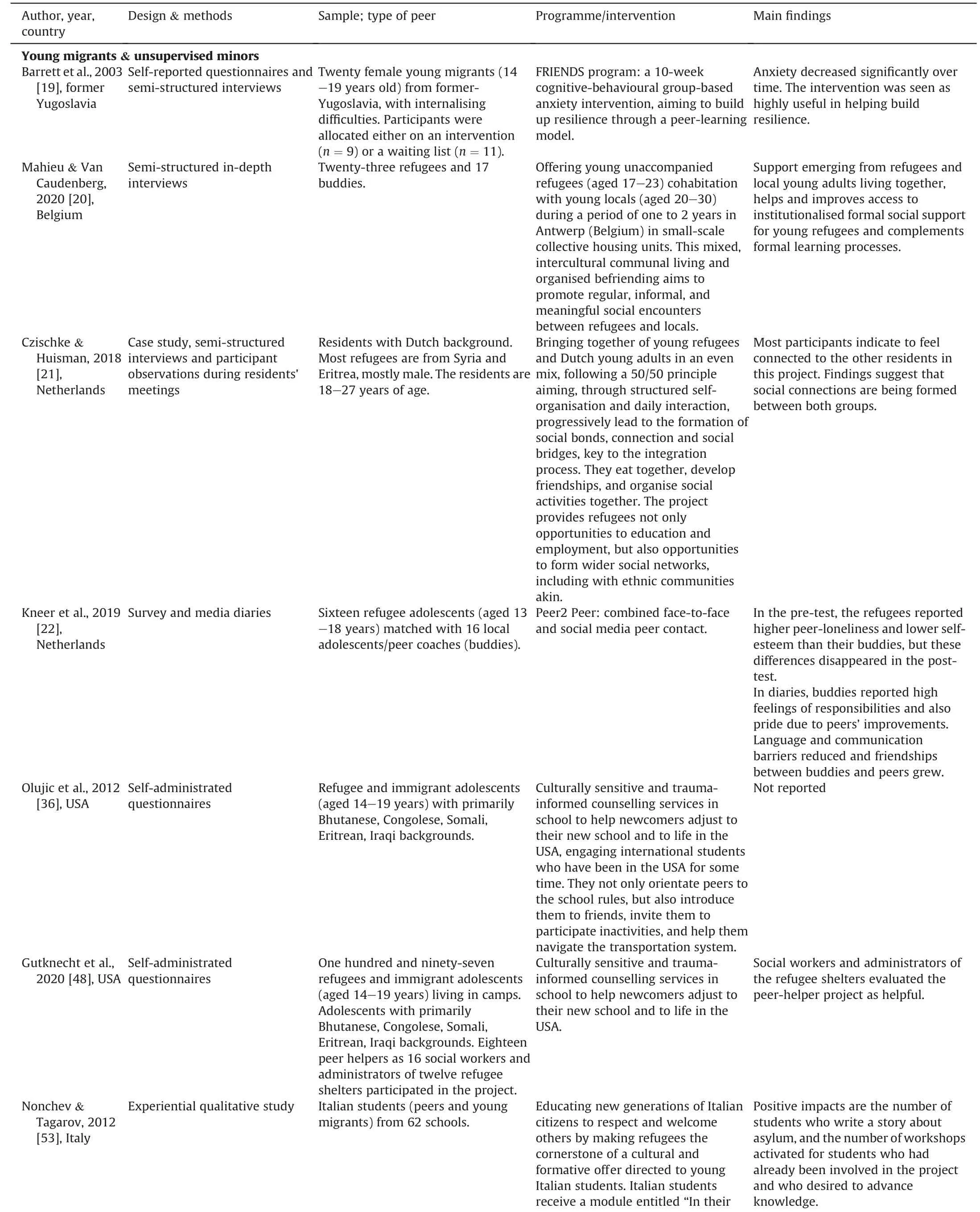
Table 1 Included studies structured per target group (n=45).
3.5.SWOT analysis
The programs/interventions (attributes) and results (consequences)are presented in Table 1 per individual target group.One study did not report outcomes.Thestrengthof the peer support method is that it provides a better quality of life outcome in the different target groups of vulnerable people,predominantly in terms of psychosocial and emotional outcomes.This applied to all the target groups apart from homeless people.Regarding weaknesses,the major obstacle seems to be the matching or the combination of compatible individuals.If the peer is not a good match with the vulnerable individual,the drop-out rate for both parties increases,and the effectiveness of the intervention decreases.Also,a mismatch or ambiguity of personal interests or intentions weakens peer support.This was mostly observed in the case of parent-child peer support.Majoropportunitiesfor peer support are giving vulnerable people the chance to have positive experiences with formal care again,offering help tailored to the individual needs of a vulnerable person,and mutual learning.Peer support also can extend,enhance,and complement professional health services.Some importantthreatsto the effectiveness of peer support are observed.First,the sustainability of the peer support projects and the commitment of volunteers are often omitted.Second,when the relationship of trust is lacking,the effects will be less positive or have less impact.Lastly,peer support should not replace any formal or professional support,that is,care provided by a health,social care,or welfare professional (Table 2).
4.Discussion
To the best of our knowledge,this is the first rapid scoping review providing a systematic and comprehensive overview of peer support initiatives among various target groups.Rodgers’ concept analysis steps and the SWOT model aided to structure and synthesise the breadth of information.As the search terms for the review were drawn up in consultation with social and health service providers,we believe to have provided an overview,fitting and informing health and social care practice and current society.Our rapid scoping review results show that peer support initiatives are not equally utilised (or not proportionally evaluated) within the different target populations.There is,for example,more evidence of peer support among foster families than among young migrants.Additionally,most of the peer support studies in our review originated from the USA.Our findings suggest a scientific underreport of peer support from countries other than the USA and certain target populations,such as homeless people.We are very aware that vulnerable groups or vulnerable individuals are difficult to reach for research purposes,depending on the nature and level of their vulnerability [64],influencing the scientific output.
According to our review,the major strength of peer support is the beneficial effect on the quality of life of vulnerable people,represented by increased emotional,social,and physical wellbeing,self-confidence,resilience,and development and use of positive coping skills.A concurrent decline in feelings of anxiety,depression,loneliness,and stress is observed.Interestingly,peer support has a two-way effect as it affects the person being supported and the peer providing the support [9].Our review shows that peer support includes mutual learning,creating an opportunity to develop new friendships,and increased feelings of responsibility and pride among peer supporters,likely to result from feelings of connection,positive interaction,and the peer’s improvements and achievements.Our findings enhance community sense and social inclusion.
Next to the positive aspects,we observed that the weakness of peer support is related to the peer’s level of involvement and commitment:too much or too little.On the one hand,the peer can be too involved and unable to ignore their interests,for instance,being a parent personally benefitting from the child’s achievements or development,affecting the non-hierarchal nature of peer support.On the other hand,the peer might lack sufficient expertise and interest in the person they are supporting or lack rapport to be adequately involved or feel involved or committed.Therefore,it seems of merit to provide peer supporters with appropriatementalizationtraining [39].In this training,peer supporters learn how to define their roles and specify(mutual)expectations for the peer and the supporter individually,or between them [39,65,66].It is known that when peers do not receive any training,preparation,or intervention,this can negatively affect the quality and content of their peer support [26].Mentalization training might enhance the sustainability of peer support initiatives by preventing burdens and strengthening peer supporters' resilience and coping skills [39].Therefore,it can be recommended to provide peer supporters with adequate training before acting as a peer supporter.
Peer support “is based on the belief that people who have faced,endured,and have overcome adversity can offersupport,encouragement,hope,and mentorship to others facing similar situations” [67].Although our review shows that peers and peer supporters without similar problems or circumstances can be a perfect match,individuals who are too similar in terms of their past experiences can become too emotionally involved to provide adequate support.Based on the review results,we cannot define or identify what constitutes an ideal peer.The studies included a variation of peer supporters.Therefore,the character and requirements of the peers in the studies very much relied on the nature of the (target) population.However,it seems clear that a bond of trust and appropriate involvement is necessary,regarded as a crucial and paramount condition for all types of peers and support [67].This again emphasises the need for training to prepare peer supporters for the challenges and barriers that might arise and to remain motivated and committed to their role as and the task of peer supporters [66,67].
Although many opportunities for peer support have been identified by the study,such as mutual learning and the possibility to tailor the interventions to the vulnerable person’s needs,peer support has its challenges.Cultural and language barriers,time,commitment issues,and high drop-out rates are being recognised to threaten the sustainability of the peer support projects.It is,therefore,of great importance to address these issues early in volunteer/peer recruitment and selection and during initiatives’development and evaluation processes.Further exploration of training or preparation programs in terms of the type of program,content,and quality would provide a better understanding of how training can contribute to sustaining peer support initiatives and encourage volunteers.Some suggestions to optimise peer support were given,including tailoring on environmental factors,matching,and specific needs of target groups[23,25].We want to emphasize that the support provided by a peer should never replace formal support.Formal and informal support should be regarded as interchangeable yet separate sources of help and support,each with unique shortcomings and benefits.Peer support,however,can act as a bridge between the vulnerable individual who has difficulties finding or asking for help and finding the right formal care or care pathway[3,5,9,31].
Additionally,during the COVID-19 pandemic,we recognised the importance of online,social media,or telephone interaction.Therefore,it would be of value to address the potential value of remotely delivered peer support and to incorporate the knowledge and expertise in peer support services during a time of social distancing.Although it is a huge challenge for online social media interventions to create an environment that enables meaningful relationships,creating a sense of belonging and a positive environment,current evidence shows that online peer support benefits vulnerable individuals in a similar way as physical,face-to-face,inperson peer support[50]although this applies to a lesser extent for people with mental health issues [46].
5.Limitations
A few shortcomings of the current study must be considered when interpreting the results.For the homeless,a limited numberof studies were available to be included,affecting to draw reliable conclusions -suggesting a knowledge gap regarding requiring more scientific efforts.One author conducted article screening,which may have introduced reporting bias,albeit common for rapid reviews [13],and group discussion and consensus followed the individual searches.The studies varied in nature,research methodology,outcome measures,and target groups.Although the data showed commonalities in strengths,weaknesses,opportunities,and threats -approached through quantitative and qualitative methods and covering a breadth of services,target groups,peers,and peer support -it is unclear how transferable the evidence is between the different contexts.Future research focusing on more homogenous types of peers and support will provide more groupspecific information.We realise that because the literature search was conducted in 2020,more up-to-date evidence has become available,so that we might have missed information.Additionally,because we did not perform a systematic review,we might have introduced bias and random error,potentially affecting validity and trustworthiness [13].
6.Conclusion
We regard this rapid scoping review as a first step to explore peer support,and we have provided an overview of various target groups.We believe that we have informed and provided information about peer support as a service provision by understanding who is exposed to peer support,who provides it,and who benefits from it.The findings can inform policymakers and strengthen existing peer systems.Peer support shows strengths and opportunities that contribute to positive effects and outcomes for the quality of life of different target groups of vulnerable people in the social,psychological,and/or physical domains.Bonds of trust and involvement are necessary to make peer support successful.Adequate and tailored training for peer volunteers to better prepare and support them throughout the engagement with their buddy is needed and requires further exploration.Attention to sustaining peer support is needed for long-term benefits and the realistic viability of projects and initiatives.By no means should peer support replace any formal or professional support,but its merit of facilitating positive experiences,though formal care (again) must be safeguarded.
Funding
This study is funded by Interreg 2 Seas Mers Zeeen (2S07-006 ENSURE).The funding organization had no role in the study design and analysis.
CRediT authorship contribution statement
Kalina Mikolajczak-Degrauwe: Validation,Formal analysis,Investigation,Writing -review &editing,Supervision,Project administration.Sybren R.Slimmen:Formal analysis,Investigation,Writing -review &editing.Dylan Gillissen: Formal analysis,Investigation,Writing -review &editing.Petra de Bil: Formal analysis,Investigation,Writing -review &editing.Valerie Bosmans: Formal analysis,Investigation,Writing -review &editing.Corrine Keemink:Formal analysis,Investigation,Writing-review&editing.Inge Meyvis: Formal analysis,Investigation,Writing -review &editing.Yvonne J.Kuipers: Conceptualization,Methodology,Validation,Funding acquisition,Writing -original draft,supervision.
Data availability statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of competing interest
There are no conflicts of interest to be reported.
Acknowledgments
We like to thank the ENSURE project partners: Health and Europe Centre;IGEMO Mechelen,Belgium;Kent County Council,Maidstone,UK;Community Centre ‘De Mussen’,The Hague,Netherlands;APEJI,Dunkerque,France,Goes City Council,Goes,Netherlands;and Community,Arques,France,for their thought and valuable comments and feedback.
Appendix A.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2023.09.002.
 International Journal of Nursing Sciences2023年4期
International Journal of Nursing Sciences2023年4期
- International Journal of Nursing Sciences的其它文章
- The associations among nurse work engagement,job satisfaction,quality of care,and intent to leave: A national survey in the United States
- 《国际护理科学(英文)》2024年征稿
- Meaning of community activity participation for older adults in couple households
- The implementation and impacts of national standards forcomprehensive care in acute care hospitals: An integrative review
- Nurse-coordinated home-based cardiac rehabilitation for patients with heart failure: A scoping review
- Effectiveness of a family-based program for post-stroke patients and families: A cluster randomized controlled trial