
术前预后营养指数对大面积烧伤患者预后的影响
2024-03-04 08:36刘延新陈华夏
新医学 2024年2期
刘延新?陈华夏

【摘要】目的 探討术前预后营养指数(PNI)对大面积烧伤患者预后的预测价值及临床意义。方法 回顾性分析56例大面积烧伤患者的临床资料,并依据临床结局将其分为存活组(n = 37)与死亡组(n = 19);收集患者的基本信息及术前1 d的相关实验室指标,使用公式计算PNI。PNI=血清白蛋白(g/L)+5×淋巴细胞(×109/L)。比较2组临床资料是否存在差异,采用单因素及多因素Logistic回归分析评价预后的影响因素;采用受试者操作特征(ROC)曲线分析术前PNI对大面积烧伤患者预后的预测价值。以术前PNI最佳截断值将患者分为高PNI组和低PNI组,采用 Kaplan-Meier法绘制生存曲线,预测2组患者术后90 d的存活率。结果 纳入研究的56例大面积烧伤患者中,术后90 d内死亡的患者为19例(33.93%)。死亡组和存活组烧伤面积、淋巴细胞及术前PNI比较差异均有统计学意义(P均< 0.05),死亡组的烧伤面积较大,淋巴细胞及术前PNI较低;2组年龄、性别、CRP、白细胞、肌酐、血小板淋巴细胞比值、白蛋白水平及有无呼吸道损伤比较差异均无统计学意义(P均> 0.05)。单因素Logistic回归分析显示,大面积烧伤患者的烧伤面积、淋巴细胞及术前PNI是影响患者死亡的危险因素;多因素 Logistic 回归分析显示,大面积烧伤患者的烧伤面积及术前PNI是影响患者死亡的独立危险因素;术前PNI预测大面积烧伤患者死亡的最佳截断值为34.45。PNI≤34.45大面积烧伤患者的90 d生存率明显低于PNI>34.45患者。结论 术前PNI与大面积烧伤患者术后90 d病死率相关。低PNI患者术后90 d生存率低于高PNI患者。识别大面积烧伤患者术前PNI水平具有重要意义,可为选择最佳手术时机提供参考,以促进创面愈合、降低烧伤患者手术后的病死率。
【关键词】烧伤;预后营养指数;大面积烧伤;病死率;营养
Effect of preoperative prognostic nutritional index on prognosis of patients with extensive burns Liu Yanxin, Chen Huaxia. Department of Burns and Plastic Surgery, Shandong Provincial Hospital Affiliated to Shandong First Medical University, Jinan 250021, China
Corresponding author, Chen Huaxia, E-mail: chx8573@163.com
【Abstract】Objective To investigate the prognostic value and clinical significance of preoperative prognostic nutritional index (PNI) in patients with extensive burns. Methods Clinical data of 56 patients with extensive burns were retrospectively analyzed, and they were divided into the survival group (n = 37) and death group (n = 19) according to clinical outcomes. Baseline data and relevant laboratory indexes at preoperative 1 d were collected. PNI was calculated using the following equation: serum albumin level (g/L) +5×total lymphocyte count (×109/L). Clinical data were statistically compared between two groups. The influencing factors of clinical prognosis were identified by univariate and multivariate Logistic regression analyses. The predictive value of preoperative PNI for clinical prognosis of patients with extensive burns was evaluated by the ROC curve. The area under the ROC curve (AUC) represents the accuracy of prediction. All patients were divided into the high and low PNI groups according to the optimal cut-off value of preoperative PNI. The survival curve was drawn by Kaplan Meier method to predict the differences in 90-d survival rate between two groups. Results Among 56 patients,19 (33.93%) died within postoperative 90 d. There were significant differences in burn area, lymphocyte count and preoperative PNI between the death and survival groups (all P < 0.05). In the death group, burn area was larger, lymphocyte count and preoperative PNI were lower than those in the survival group. There were no significant differences in age, sex, CRP, white blood cell count, creatinine, PLR, albumin levels and the incidence of respiratory tract injury between two groups. Univariate Logistic regression analysis showed that burn area, lymphocyte count and preoperative PNI were the risk factors of death. Multivariate Logistic regression analysis indicated that burn area and preoperative PNI were the independent risk factors for death. The optimal cut-off value of preoperative PNI to predict death in patients with extensive burns was 34.45. The 90-d survival rate of patients with PNI≤34.45 was significantly lower than that of their counterparts with PNI>34.45. Conclusions Preoperative PNI is associated with 90-d death rate in patients with extensive burns. The 90-d survival rate of patients with low PNI is lower than that of those with high PNI. These findings indicate that it is of significance to identify preoperative PNI for patients with extensive burns, which can provide reference for selecting the optimal timing for surgery, accelerate wound healing and reduce the death rate of patients with extensive burns.
【Key words】Burn; Prognostic nutritional index; Extensive burn; Death rate; Nutrition
与锐器伤、挤压伤等常见外伤不同,烧伤创面的愈合过程具有明显的特殊性[1]。烧伤创面基本不存在出血期,而细胞增殖与组织重塑的周期明显长于一般外伤,烧伤后机体处于高代谢状态,大面积烧伤患者的静息能量消耗明显高于正常水平,对营养物质的需求也更加旺盛[2-3]。因此,营养相关指标对评估大面积烧伤患者病情严重程度及预后具有重要意义。预后营养指数(PNI)是基于患者的血清白蛋白水平和淋巴细胞来评价患者围手术期营养状况及预后的指标[4]。PNI被广泛应用于临床,不仅可以评估消化道肿瘤患者的预后,还与游离皮瓣移植、高血压性脑出血、心力衰竭和肾移植患者的不良结局有关[5-9]。而PNI在烧伤领域的应用较少,既往的研究表明,术前PNI水平会影响大面积烧伤患者米克(MEEK)植皮术的成活率,而术后PNI水平会影响老年烧伤患者的预后[10-11]。本研究的目的是探讨术前PNI 对大面积烧伤患者预后的影响,并找出最佳截断值,以期为烧伤患者的治疗提供参考。
对象与方法
一、研究对象
回顾性分析2015年1月至2022年8月在山东省立医院烧伤整形外科住院治疗的56例大面积烧伤患者的临床资料。纳入标准:①烧伤总面积≥50%;②受伤后48 h内就诊于我院的热力烧伤患者;③入院前未行清创手术治疗。排除标准:①年龄<18岁者;②非医嘱离院的患者;③住院期间未接受手术治疗的患者;④受伤前合并高血压、糖尿病、心脏病等基础疾病者。观察大面积烧伤患者从第一次手术后90 d内的临床预后情况,根据其预后分为存活组(n = 37)与死亡组(n = 19)。收集患者的年龄、性别、烧伤面积、是否有吸入性损伤、术前1 d的CRP、白细胞、肌酐、血小板与淋巴细胞比值、白蛋白水平及淋巴细胞,并计算患者术前PNI。PNI=血清白蛋白(g/L)+5×外周血淋巴细胞总数(×109/L)[4]。本研究经医学伦理委员会审批(批件号:2023-613),所有患者均知情同意。
二、治疗方案
大面积烧伤患者入院后的治疗方案基本一致:①积极补液、抗休克、控制感染、创面规律换药;②对轻度吸入性损伤患者采用氧疗、雾化等治疗,对中度及重度的患者酌情进行气管切开、呼吸道灌洗、机械通气等呼吸支持治疗;③对于四肢、胸腹部及颈部环形焦痂形成时,早期行切开减张;④待患者平稳度过休克期后,择期行创面清创及植皮手术;⑤术后创面规律换药,对症支持治疗。
三、统计学处理
用SPSS 22.0软件进行数据分析,符合正态分布的计量资料均以表示,采用独立样本t检验;不符合正态分布的计量资料以M(P25,P75)表示,采用Wilcoxon秩和检验;计数资料组间比较采用χ 2
检验。对2组有差异的数据进行单因素及多因素Logistic回归分析;通过绘制受试者操作特征(ROC)曲线来评估PNI的灵敏度及特异度,并通过计算约登指数来决定PNI的最佳截断值。以最佳截断值分为高PNI组和低PNI组,Kaplan-Meier法绘制生存曲线,预测术后90 d的存活率。P <
0.05为差异有统计学意义。
结果
一、一般资料
本研究共纳入56例大面积烧伤患者,其中男49例、女7例;在纳入研究的患者中,第一次手术后90 d內的死亡的患者为19例,占33.93%。死亡组和存活组烧伤面积、淋巴细胞及术前PNI比较差异均有统计学意义(P均< 0.05),死亡组的烧伤面积较大,淋巴细胞及术前PNI较低;2组年龄、性别、CRP、白细胞、肌酐、血小板淋巴细胞比值、白蛋白水平及有无呼吸道损伤比较差异均无统计学意义(P均> 0.05)。见表1。
二、单因素及多因素Logistic回归分析
将上述存在统计学差异的变量纳入单因素Logistic回归分析显示,大面积烧伤患者的烧伤面积、淋巴细胞及术前PNI是影响患者死亡的危险因素(P均< 0.05);将上述危险因素纳入多因素Logistic回归分析显示,大面积烧伤患者的烧伤面积和术前PNI是影响患者预后的独立危险因素(P均< 0.05)。见表2、3。
三、术前PNI预测大面积烧伤患者死亡的最佳截断值
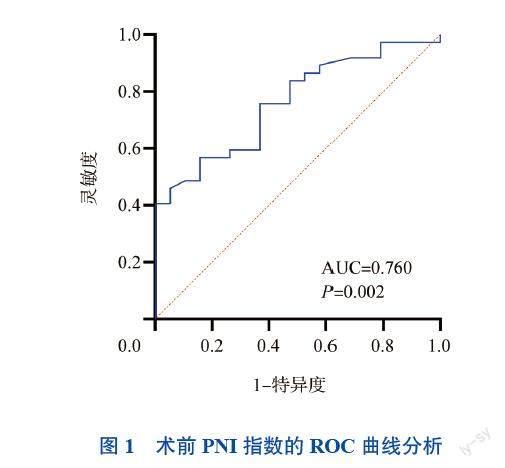
以大面积烧伤患者术后90 d是否生存为结局指标,绘制术前PNI的 ROC 曲线,曲线下面积为0.760(95%CI为0.635~0.885,P = 0.002),最佳临界值为34.45,对应的灵敏度为56.8%,特异度为84.2%。见图1。
四、大面积烧伤患者术后90 d生存率的Kaplan-Meier曲线
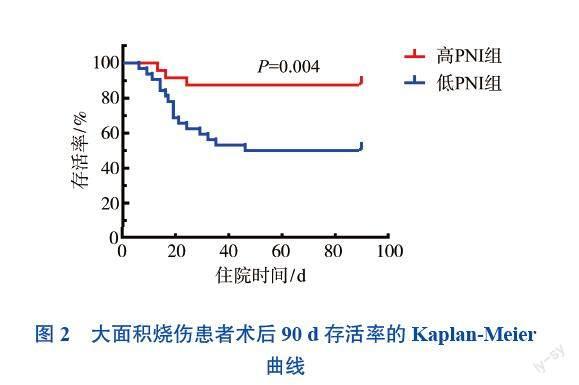
根据PNI最佳截断值将患者分为高PNI组和低PNI组,绘制大面积烧伤患者术后90 d生存率的Kaplan-Meier曲线,结果显示PNI ≤34.45的大面积烧伤患者的90 d存活率明显低于PNI>34.45患者(P = 0.004)。见图2。
讨论
烧伤的发病机制包括热力烧伤、化学烧伤、电烧伤及放射性烧伤等,而热力烧伤占烧伤的大多数[12]。由于液体复苏、抗生素治疗、外科手术和营养支持治疗等技术的发展,烧伤患者的病死率有所下降,但仍处于较高水平。大面积烧伤的高病死率不仅是由于低血容量性休克和感染,还归因于免疫抑制、过度炎症和代谢亢进等异常的机体反应[13-15]。有证据表明,炎症与分解代谢细胞因子的产生增加、肌肉分解代谢增加,以及白蛋白水平降低存在相关关系,营养不良可能是炎症的替代指标[16]。因此,评估患者的营养状况对于烧伤患者的预后具有非常重要的意义。
PNI由日本学者小野寺等提出,最初是用以评估外科患者的术前营养状况、术中风险及术后的预后状况。PNI根据血清白蛋白水平和淋巴细胞计算得来,血清白蛋白水平可以评估烧伤患者的营养和炎症反应状态,持续的低蛋白血症可以明显影响烧伤患者病情的严重程度[17]。淋巴细胞在免疫应答中起关键作用,大面积烧伤后淋巴细胞水平和功能发生重大变化,淋巴细胞早期减少反映患者预后不良[18-19]。因此,与术后的相关指标相比,术前PNI既是一种营养指标,也是一种免疫和炎症指标,可以更有效地反映烧伤患者高分解代谢状态下引起的营养不良和免疫抑制状态。PNI对评价烧伤患者预后的价值在国内尚无研究报道。因此,本研究着重探讨术前PNI对大面积烧伤患者预后的影响。
本研究多因素 Logistic 回归分析显示,烧伤面积及术前PNI是影响大面积烧伤患者预后的独立危险因素。术前PNI与大面积烧伤患者预后间的作用机制尚不完全清楚,先前的研究报道了几种潜在的机制。首先,血清白蛋白在氨基酸化合物和脂肪酸的运输以及创面愈合中起着关键作用。白蛋白水平降低会增加伤口感染的风险,导致伤口愈合缓慢,免疫力降低,从而影响烧伤患者的预后[20]。其次,淋巴细胞在机体免疫反应中起重要作用。创伤性损伤和脓毒症后未能重建正常淋巴细胞也与病死率增加有关。烧伤后机体的应激状态会引发一系列病理生理反应,代谢需求增加,导致营养物质代谢速率大幅提高[21]。由此引发的营养不良会进一步导致免疫功能被抑制,患者创面愈合时间延长,死亡风险增加[22]。因此,术前PNI降低反映了机体营养不良状态和抵抗炎症反应及感染的保护功能降低,从而影响大面积烧伤患者的预后。
本研究中预测大面积烧伤患者术后90 d病死率的术前PNI最佳截断值为34.45,与先前的研究类似[14]。然而,研究得到的PNI最佳截断值远低于其他领域的研究。例如,影响胃癌患者术后生存率及复发率的术前PNI最佳截断值约为45[23]。黄平等(2021年)研究显示,预测支气管扩张急性加重期患者疾病严重程度的PNI最佳阈值是49.67和45.94。烧伤患者和其他疾病患者间临界值的差异可能是由于烧伤的特殊性决定的。对于大面积烧伤患者,热力烧伤导致组织破坏,可伴有毛细血管渗漏、水肿形成和严重循环血容量不足,液体复苏时大量使用晶体液也可引起血液稀释,从而导致低白蛋白血症。此外,烧伤患者的皮肤屏障受损,免疫系统受到抑制,淋巴细胞数量下降。因此,用于预测大面积烧伤患者术后病死率的术前PNI最佳截断值可能相对其他疾病偏低。
综上所述,术前低PNI(≤34.45)是影响大面积烧伤患者预后的独立危险因素,这可能为确定手术时机提供参考。在条件允许的情况下,手术时机应当推迟到患者得到足够的营养支持后进行,以改善患者的一般情况,促进创面愈合,改善预后。然而,本研究是一项单中心回顾性研究,因回顾性研究中的影响因素无法控制,将不可避免的产生偏倚;其次,本研究样本为单中心数据,样本量也可能对结果的准确性产生一定影响。期待进一步多中心、大样本和前瞻性的研究。
参 考 文 献
[1] 孙勇, 彭曦. 重视烧伤创面愈合中的蛋白质营养问题[J]. 肠外与肠内营养, 2022, 29(2): 65-68.
Sun Y, Peng X. Pay attention to protein nutrition in burn wound healing[J]. Parenter Enter Nutr, 2022, 29(2): 65-68.
[2] 贾赤宇, 王鹏, 张泽鑫. 重症烧伤救治:理念、挑战与希望[J]. 中华损伤与修复杂志(电子版), 2021, 16(5): 374-382.
Jia C Y, Wang P, Zhang Z X. Treatment of severe burns: concept, challenge and hope[J]. Chin J Inj Repair Wound Heal (Electron Ed), 2021, 16(5): 374-382.
[3] 李嵩, 張森林. 早期肠内营养治疗大面积重度烧伤患者疗效分析[J]. 中国烧伤创疡杂志, 2021, 33(6): 395-398.
Li S, Zhang S L. Efficacy analysis of early enteral nutrition in the treatment of extensive severe burns[J]. Chin J Burns Wounds Surf Ulcers, 2021, 33(6): 395-398.
[4] Onodera T, Goseki N, Kosaki G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients[J]. Nihon Geka Gakkai Zasshi, 1984, 85(9): 1001-1005.
[5] Yang Y, Gao P, Song Y, et al. The prognostic nutritional index is a predictive indicator of prognosis and postoperative complications in gastric cancer: a meta-analysis[J]. Eur J Surg Oncol, 2016, 42(8): 1176-1182.
[6] Yu J, Hong J P, Suh H P, et al. Prognostic nutritional index is a predictor of free flap failure in extremity reconstruction[J]. Nutrients, 2020, 12(2): 562.
[7] 唐渊. 预后营养指数与高血压性脑出血术后30天病死率的关系[J]. 中国医师进修杂志, 2018, 41(1): 30-33.
Tang Y. Relationship between prognostic nutritional index and 30-day mortality after operation in patients with hypertensive intracerebral hemorrhage[J]. Chin J Postgrad Med, 2018, 41(1): 30-33.
[8] Shirakabe A, Hata N, Kobayashi N, et al. The prognostic impact of malnutrition in patients with severely decompensated acute heart failure, as assessed using the Prognostic Nutritional Index (PNI) and Controlling Nutritional Status (CONUT) score[J]. Heart Vessels, 2018, 33(2): 134-144.
[9] Hori S, Ichikawa K, Morizawa Y, et al. Clinical significance of postoperative nutritional status as a prognostic factor in kidney transplant recipients[J]. Transplant Proc, 2019, 51(6): 1763-1772.
[10] Hu G, Yuan L, Peng Y, et al. Predictive value of the prognostic nutrition index for the prognosis of patients with severe burns treated with the meek graft[J]. J Burn Care Res, 2021, 42(3): 448-453.
[11] Seo Y J, Kong Y G, Yu J, et al. The prognostic nutritional index on postoperative day one is associated with one-year mortality after burn surgery in elderly pa-tients[J]. Burns Trauma, 2021, 9: tkaa043.
[12] Jeschke M G, van Baar M E, Choudhry M A, et al. Burn injury[J]. Nat Rev Dis Primers, 2020, 6(1): 11.
[13] Xiao W, Mindrinos M N, Seok J, et al. A genomic storm in critically injured humans[J]. J Exp Med, 2011, 208(13): 2581-2590.
[14] Stanojcic M, Abdullahi A, Rehou S, et al. Pathophysiological response to burn injury in adults[J]. Ann Surg, 2018, 267(3): 576-584.
[15] Jeschke M G, Gauglitz G G, Kulp G A, et al. Long-term persistance of the pathophysiologic response to severe burn injury[J]. PLoS One, 2011, 6(7): e21245.
[16] Raposeiras Roubín S, Abu Assi E, Cespón Fernandez M, et al. Prevalence and prognostic significance of malnutrition in patients with acute coronary syndrome[J]. J Am Coll Cardiol, 2020, 76(7): 828-840.
[17] Findik O, Aydin U, Baris O, et al. Preoperative low serum albumin levels increase the requirement of renal replacement therapy after cardiac surgery[J]. Heart Surg Forum, 2016, 19(3): E123-E127.
[18] Girardot T, Rimmelé T, Venet F, et al. Apoptosis-induced lymphopenia in sepsis and other severe injuries[J]. Apoptosis, 2017, 22(2): 295-305.
[19] Osuka A, Ishihara T, Shimizu K, et al. Natural kinetics of blood cells following major burn: impact of early decreases in white blood cells and platelets as prognostic markers of mortality[J]. Burns, 2019, 45(8): 1901-1907.
[20] Hu G, Yuan L, Peng Y, et al. Predictive value of the prognostic nutrition index for the prognosis of patients with severe burns treated with the meek graft[J]. J Burn Care Res, 2021, 42(3): 448-453.
[21] 羅月, 黎宁. 严重烧伤患者早期肠内营养治疗的研究进展[J]. 中华烧伤杂志, 2021, 37(9): 880-884.
Luo Y, Li N. Research advances on early enteral nutritional therapy in severe burn patients[J]. Chin J Burns, 2021, 37 (9): 880-884.
[22] 贺荣鹏. 早期肠内、肠外强化营养支持在特大面积危重烧伤救治中的疗效分析[J]. 中国现代药物应用, 2020, 14(5): 200-202.
He R P. Analysis of the curative effect of early enteral and parenteral nutrition support in the treatment of severe burns in large area[J]. Chin J Mod Drug Appl, 2020, 14(5): 200-202.
[23] Maejima K, Taniai N, Yoshida H. Assessment of the prognostic nutritional index as a prognostic factor for the progression and recurrence of gastric cancer progression and recurrence[J]. J Nippon Med Sch,2022,89(5):487-493.
(收稿日期:2023-09-25)
(本文编辑:杨江瑜)
猜你喜欢
临床骨科杂志(2022年3期)2022-11-24
今日农业(2021年11期)2021-08-13
现代畜牧科技(2021年4期)2021-07-21
中国生殖健康(2019年8期)2019-01-07
幸福(2018年33期)2018-12-05
中国实用医药(2016年23期)2016-12-26
中国当代医药(2016年28期)2016-12-20
中国实用医药(2016年28期)2016-12-07
中国实用医药(2016年24期)2016-10-17
海峡姐妹(2016年5期)2016-02-27
