
Combined laparoscopic and endoscopic method for foreign body removal from descending colon: A case report
2024-03-27 08:11KhairunnisaCheGhazaliHuzairiYaacobAhmadShanwaniMohamedSidek
Khairunnisa Che Ghazali,Huzairi Yaacob,Ahmad Shanwani Mohamed Sidek
Abstract BACKGROUND The majority of published reports on foreign bodies (FBs) involve the rectum and applied a transanal retrieval.Usually,patients with FB above the rectum are subjected to laparotomy for removal.Here,we illustrate the case of a man with an FB that had migrated into the descending colon,and its successful removal via a laparoscopic approach.CASE SUMMARY A 43-year-old man,who had the habit of FB insertion into his anus to aid defecation,presented upon experience of such an FB slipping through and migrating upward to the distal colon.Plain abdominal radiograph revealed a bottle-shaped FB,positioned in the left iliac fossa region.The FB was successfully removed via a laparoscopic-assisted procedure in which we combined diagnostic laparoscopic and endoscopic techniques during surgery.The patient was monitored for 2 d postoperatively and subsequently discharged home.CONCLUSION A minimally invasive approach should be adopted to aid extraction of colorectal FB as it is effective and safe.
Key Words: Foreign body;Colorectal;Laparoscopic approach;Removal technique;Minimally invasive;Case report
INTRODUCTION
The majority of published literature on foreign bodies (FBs) involves the rectum and transanal retrievals.However,if the FB dislodges above the rectum,the retrieval success rate drops and an operative intervention,most frequently laparotomy,may be required[1].
Herein,we describe the case of a man who presented with an anally-inserted FB that had migrated into the descending colon,and its successful removalviaa laparoscopic approach.Minimally invasive approaches offer great advantages over open surgery,in terms of holistic impact on the abdominal cavity,shorter hospital stays,and earlier recovery[2].
CASE PRESENTATION
Chief complaints
A 43-year-old man was referred for FB in the sigmoid colon.
History of present illness
For the past 5 yr,the patient had experienced chronic constipation requiring straining and digitation,and resulted in a once-weekly passing motion.He also had a propensity of inserting unusual FB anally in order to dilate his anus and ease his defecation.He had no history of changed bowel habits or tenesmus,nor a family history of cancer.
Two days before hospitalisation,he had purposefully placed a shampoo bottle inside his anus to aid defecation.Unfortunately,the bottle slipped through deeper and entered the intestinal lumen.He had attempted to remove it but was unsuccessful.He stated that he sought treatment at our facility following the development of abdominal pain and subsequent personal concern about a retained FB.
History of past illness
The patient’s past medical history was irrelevant.
Personal and family history
The patient had no significant personal or family history.
Physical examination
The patient’s abdomen was soft on palpation,and there was no peritonism.A vague lump could be felt above the left iliac fossa region.On digital rectal examination,we were unable to feel the FB.
Laboratory examinations
All within normal range.
Imaging examinations
Plain abdominal radiograph revealed a bottle-shaped FB,positioned in the left iliac fossa region,correlating with the clinical history and examination findings (Figure 1).No free air was noted.

Figure 1 Plain abdominal radiograph showed bottle-shaped foreign body in the left sided of abdomen (orange arrow).
FINAL DIAGNOSIS
Retained FB in descending colon.
TREATMENT
The patient consented to examination under anaesthesia,including laparoscopic assessment.The laparoscopic-assisted procedure itself involved a 12-mm infraumbilical camera port and another two 5-mm working ports placed at the right iliac fossa and left lumbar under direct vision.During the laparoscopy,a bulging FB was noted at the descending colon.The bowel wall appeared normal (Figure 2).There was congenital adhesion at the descending-sigmoid junction and the lateral abdominal wall,causing angulation;hence,adhesiolysis was performed to straighten the axis (Figure 3).We then applied a laparoscopic bowel grasper and Babcock forceps to assist in milking down the FB from the sigmoid colon to the rectum (Figure 4).A surgeon manipulated the bowel with the traction and counter-traction method,until it reached the rectum (Figure 5).

Figure 2 Laparoscopic view of sigmoid colon. A and B: Following the shape of foreign body.The sigmoid colon serosa was normal looking and non edematous.
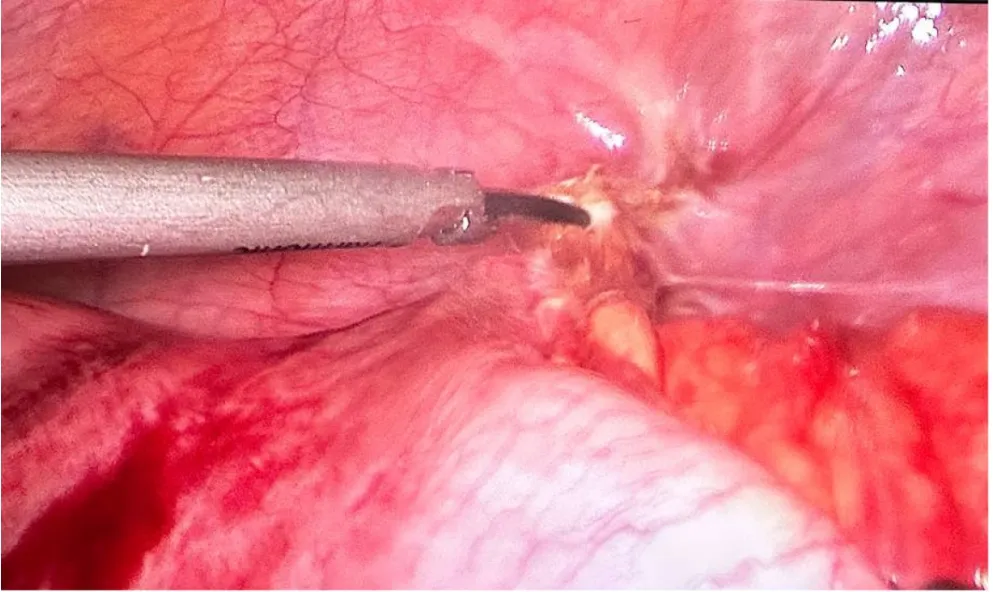
Figure 3 Adhesiolysis performed to release adhesion to straighten the axis.

Figure 4 Surgical diagram. A and B: A 5-mm laparoscopic atraumatic bowel grasper and babcock forcep were used to help pushed down the foreign body into the rectum,with traction and counter-traction methods.

Figure 5 Surgical diagram. A and B: The foreign body managed to pass down into the rectum.
No proper bowel preparation was made.We only performed a gentle on-table rectal wash-out,to clean the rectum.Following that,we performed a sigmoidoscopy,to visualize the colonic mucosa and the FB in the rectum.The rectal mucosa was not inflamed nor oedematous (Figure 6).To facilitate the extraction,the bimanual manipulation technique was applied.Gentle suprapubic pressure was applied by a second surgeon andviaa transanal approach to retrieve the bottle.Meanwhile,the first surgeon pushed the FB toward the anusvialaparoscopy until it reached the second surgeon’s hand in the anus (Figure 7).Once the bottom of the bottle could be felt,it was grasped by the second surgeon’s fingers and fully pulled out.A 14 cm × 4 cm green-coloured plastic shampoo bottle was removed successfully (Figure 8).

Figure 6 The rectal mucosa was not inflamed nor oedematous. A: The assistant is doing sigmoidoscopy;B: Endoscopic image of rectum,with greenish foreign body (white arrow).

Figure 7 The first surgeon pushed the FB toward the anus via laparoscopy until it reached the second surgeon’s hand in the anus. A:Bimanual palpation of foreign body via suprapubic and transanally;B: Successful retrieval of the foreign body.
Figure 9 shows the port placement wound postoperatively.

Figure 9 Port placement area. Blue arrow: 12-mm camera port at infraumbilical.Orange arrow: 5-mm working at right iliac fossa and left lumbar.
OUTCOME AND FOLLOW-UP
The patient was monitored for 2 d postoperatively and subsequently discharged to home.Prior to discharge,he was referred to the psychiatric unit to elicit any diagnosis on psychiatric illness underlying this abnormal habit.Based on the psychiatric assessment,his behaviour was mainly attributed to his constipation,and a plan was made to follow-up with manometry and biofeedback.
DISCUSSION
Despite being underreported,colorectal FBs occur frequently[1].Usually,a patient suffering from colorectal FB will present late after the lodging episode,when they fail attempt(s) to remove it;this is typically due to embarrassment and a perception of taboo[1].The reasons for colorectal FB insertion are varied and include underlying psychiatric illness,selfadministration to alleviate a symptom of anorectal disease,for sexual gratification or autoeroticism,from a criminal assault,for drug trafficking,or as a relatively mundane medical manoeuvre (e.g.,thermometer or enema insertion)[3-5].Objects recorded in case reports are toys,bottles,light bulbs,glasses,fruits,and vegetables[6,7].
Eftaihaetal[5] simplified the classification of retained FB by dividing them into low-lying or high-lying,which then dictates the clinical approach for removal.For low-lying FB,the mass can be palpated in the rectal ampulla;for high-lying FB,the mass is proximal to the rectosigmoid junction.FBs retained in the rectum can usually be managed with a transanal removal at bedside;sometimes,the case may require appropriate anaesthesia[8].If the FB becomes dislodged cranially,operative intervention is usually required[6,8],and in the presence of peritonism,emergency laparotomy is necessitated[1,3,7].In the case of a stable patient with no need for urgent surgery,sedation and attempt at bedside extraction should be performed[5,8].
A retrospective study by Coskunetal[6] evaluated 15 patients with FB in rectum who were treated in Izmir,Turkey over a 10-yr period.The rectal FBs were removed transanally under general anaesthesia from 12 of the patients,while the remaining 3 required laparotomy.Kimetal[2] performed a retrospective study of 14 Korean patients with retained FBs,from January 2006 to December 2018.Among these patients,2 had removal of the FB in the emergency department,12 underwent general anaesthesia for anal sphincter relaxation,and 5 had FB retrieved transanally.The remaining 7 patients had laparotomy,with 2 needing colonic milking only,4 requiring colotomy and repair,and 1 necessitating Hartman’s procedure due to faecal peritonitis.
In our patient,who presented with a retained FB after 3 d,the possibility of a successful transanal extraction was minimal.In some circumstances,choosing the best treatment approach can be difficult.Knowing that the FB was a shampoo bottle,and it is quite large,hence endoscopic retrieval alone may not be adequate since we know that endoscopic equipment to retrieve specimen is small for example the Roth Net retrieval device.Hence,the patient was therefore subjected to laparoscopic assessment as well.Many advantages of laparoscopy surgery in the treatment of FB removal.It allows assessment of intraperitoneum,in this case we can assess large bowel condition with just a keyhole wound.In our case,combination approach was suitable because firstly,this is because the FB was trapped higher up,at the descending colon area.Secondly,we speculated the affected bowel was probably inflamed,thickened,and oedematous.Thirdly,there was a possibility of a stricture or stenotic bowel lumen distally either due to angulation or repetitive injuries.The majority of centres approach failed-extraction FB cases with laparotomy[8].Rispolietal[8] first described the combined laparoscopic and endoanal approach applied successfully to remove an FB from distal colon.In general,a minimally invasive approach offers greater advantage,in terms of facilitating holistic evaluation of abdominal cavity,shorter hospital stays,and early recovery after surgery[1].Some surgeons have also described laparoscopy as an aid to push the object distally,but no cases described in the literature have included a comparison of this technique to conventional treatment.Generally,using laxative as medical treatment to help expel FB is not recommended.
In most cases,close observation is adequate as postextraction management.However,some authors have suggested sigmoidoscopy assessment to evaluate mucosal laceration,bleeding,or perforation[1,6,7].Follow-up,in general,is suggested for assessing long-term complications,such as incontinence,stenosis,or fistula[1,3,6].
CONCLUSION
In conclusion,the colorectal surgeon should be familiar with various extraction methods.A minimally invasive approach should be the way forward,as it has also been shown to be safe in aiding extraction of colorectal FB.Another approach that can be explored is the hand-assisted laparoscopic (otherwise known as HAL) technique.
FOOTNOTES
Author contributions:Che Ghazali K was the patient’s surgeon,collected the data,wrote the manuscript,and performed the literature search;Yaacob H was the patient’s surgeon and reviewed the manuscript for accuracy;Mohamed Sidek AS reviewed the manuscript for scientific accuracy.
Informed consent statement:All study participants,or their legal guardian,provided informed written consent prior to study enrollment.
Conflict-of-interest statement:The authors declare that they have no conflicts of interest related to this case or its publication.
CARE Checklist (2016) statement:The authors have read the CARE Checklist (2016),and the manuscript was prepared and corrected according to the CARE Checklist (2016).
Open-Access:This article is an open-access article that was selected by an in-house editor and fully peer-reviewed by external reviewers.It is distributed in accordance with the Creative Commons Attribution NonCommercial (CC BY-NC 4.0) license,which permits others to distribute,remix,adapt,build upon this work non-commercially,and license their derivative works on different terms,provided the original work is properly cited and the use is non-commercial.See: https://creativecommons.org/Licenses/by-nc/4.0/
Country/Territory of origin:Malaysia
ORCID number:Khairunnisa Che Ghazali 0000-0003-0990-5060;Huzairi Yaacob 0009-0009-2681-9640.
S-Editor:Gao CC
L-Editor:A
P-Editor:Zhao YQ