
Topography versus non-topography-guided photorefractive keratectomy with corneal cross-linking variations in keratoconus
2022-05-15 05:40SanaNiaziJorgeAliodelBarrioAzadSanginabadiFaridehDoroodgarCyrusAliniaAlirezaBaradaranRafiiFeaizollahNiaziHosseinMohammadRabeiMohammadMehdiSadoughiJorgeAlio
INTRODUCTION
Effective therapy for corneal ectatic diseases, such as iatrogenic corneal ectasia, keratoconus, and pellucid marginal degeneration, involve confronting two specific parameters: the corneal optical deficiency and the biomechanical inconsistency of the irregular cornea
. Contact lenses have corrected patients with irregular astigmatism for years (scleral lenses and rigid gas permeable contact lenses) in mild cases of keratoconus, and penetrating keratoplasty has been the surgical option in severe cases. Other effective surgical methods are now being used, such as intracorneal ring segments and deep anterior lamellar keratoplasty while other approaches were proposed and attempted in the past, such as conductive keratoplasty and epikeratophakia
.
在学习函数综合应用知识时,可以引发学生思考其图象(有无交点、交线围成的图形面积、数形结合等),也可以通过多媒体向学生展示不同函数所表示的图象,学生通过这些图象的变换很快就能理解函数的概念了.除了多媒体教学,教师还可以组织学生参加动手绘画等有趣的活动来学习数学.综上所述,高中数学的教学应该有意识、有目的、有策略地针对学生逻辑思维能力培养的需要进行变通,让学生在日常生活中养成逻辑思维的习惯,以此提高高中数学教学效率、促进学生学习效率的提高.
Corneal collagen cross-linking (CXL) opened a new horizon in the effective treatment of progressive corneal ectasia
.The blend of ultra-violet A and riboflavin as a light sensitivity factor produced inter-fibrillary connection between cornea stromal collagen fibers, and as a result, decreased corneal deformability, corneal resistance, and stabilized keratoconus
.With CXL, the issue of biomechanical instability has been effectively confronted, as indicated by the confirmation that CXL has been successful in stopping the progression of ectatic disorders
.
射频模块采用5 V 外部供电,其主要供电需求为3.3 V和5 V,可分为控制部分和下变频变频部分。控制部分仅仅是STC15W408S控制器的电源,采用通用的LM1117-3.3稳压到3.3 V。下变频变频部分电源涉及到低噪声放大器、锁相环、混频器等噪声敏感器件的供电,需要选择高文波抑制比的低压差稳压器[31]。MIC5245系列与MIC5205系列专为射频器件稳压而设计,采用该两个系列作为射频部分的稳压器件。图8展示了系统部分电源网络。
[21] Richardson H W., “Economies and Diseconomies of Agglomeration”, in Urban Agglomeration and Economic Growth, Springer Berlin Heidelberg, 1995, pp. 123-155.
However, the visual outcomes and the topography of patients treated only by CXL demonstrate no change or insignificant change due to remaining irregular astigmatism. Excimer laser surgery in the form of non-topography-guided and topographyguided photorefractive keratectomy, besides decreasing irregular astigmatism, changes the shape of the cornea improving visual outcomes
. The combination of CXL with excimer laser photorefractive keratectomy has recently gained interest in treating mild to moderate keratoconus
. However, there is still no evidence confirming the potential benefits of topography-guided photorefractive keratectomy method over standard, non-topograph-guided photorefractive keratectomy.This study aims to compare and appraise the visual outcomes of topography and non-topography-guided photorefractive keratectomy with sequential and simultaneous CXL in keratoconus patients.
SUBJECTS AND METHODS
The study received approval from the local ethics committee (IR. SBMU. RETECH.RECH.1400.1216).As a standard protocol, all surgeries were performed by one surgeon (Doroodgar F) after obtaining appropriate written consent from a trained, certified good clinical practice (GCP)examiner.
This prospective study included four groups of keratoconus patients: Sequential topographyguided photorefractive keratectomy with CXL (sequential TGPRK, 19 eyes/10 patients), simultaneous topography-guided photorefractive keratectomy with CXL (simultaneous TGPRK, 15 eyes/8 patients), simultaneous non-topography guided photorefractive keratectomy with CXL (simultaneous non-TG-PRK, 17 eyes/9 patients), and sequential non-topography guided photorefractive keratectomy with CXL (sequential non-TG-PRK, 18 eyes/9 patients). The patients were treated between January 2014 and October 2015.
Inclusion criteria for the study focused on patients over 34y(range from 34 to 41y) with stable corneal topography and refraction for at least six months and an estimated residual bed thickness of >410 μm.
9月23日18时,杜家台分洪闸开始关闭闸门,历时5分50秒全部关闭完毕。整个分流期间,杜家台分洪闸共开启53小时36分,共分流汉江下游超额洪水约2亿m3,有效降低仙桃以下河段水位约0.6m,减少仙桃站超保证水位时间50小时。
CXL increases the level of entombed fibrillar linkages enhancing the biomechanical quality of the cornea. Many investigations have confirmed the effective stabilization of keratoconus progression after CXL
. Almost all previous studies have proven that TG-PRK and non-TG-PRK with sequential, and simultaneous CXL are effective and safe and result in good visual performance in keratoconus eyes
. Most studies have reported that simultaneous treatment (TG-PRK and non-TG-PRK followed immediately by CXL) produces excellent results compared to sequential treatment
, and other studies have not indicated a difference between these two methods
. Efficacy and safety of simultaneous and sequential methods would enhance the refractive condition of the eye
.To our knowledge, this is the first study to compare four surgical methods in keratoconus patients. The comparison aims to determine the best method to treat patients with keratoconus and evaluate functional and consistent outcomes. Achieving useful vision comprises enhancing UCVA and BCVA and standardization of corneal topography, demonstrating that these patients are less subject to contact lens use. Therefore, a higher postoperative visual quality would be achieved.
成本信息数据库是将项目的历史数据进行沉淀。该数据库平台主要用于成本核对,为投资、拿地决策提供信息,为供应商选择,甚至是项目实施过程中的变更和认质认价提供依据。采用人工智能的方式建立成本信息平台,而不是简单地依赖成本工程师的个人经验,这是大数据时代的必然发展趋势。
Preoperative examinations were uncorrected and best-corrected distance visual acuity (UCVA and BCVA)applying a standard Snellen eye chart, cycloplegic refraction with cyclopentolate 1.0%, contrast sensitivity exam under mesopic (3 cd/m
) and photopic (85 cd/m
) conditions using the CVS1000 contrast sensitivity exam (VectorVision, Greenville,SC, USA) manifest refraction, slit-lamp biomicroscopy of the anterior and posterior segment evaluation, Scheimpflug imaging with the Pentacam HR device (Oculus Surgical, Inc.,USA), and intraocular pressure measurements for each group separately. Contact lens users were instructed to stop wearing contact lenses for about fourteen days before being screened in the case of soft contact lens users and a month before being screened in the case of rigid gas permeable or scleral contact lenses. The patients were examined for 1, 3, and 6y after the surgery. All postoperative follow-ups included a measurement of UCVA and BCVA, contrast sensitivity, and refraction.
拼音作为小学阶段语文课程教育教学的基础,同时也是学生学习更高层次知识的过渡,而且关系学生的日后自主学习与生活。拼音教学的重要性不言而喻,创新和改进拼音教学方法势在必行。
Surgical Technique
The restrictive programming in the Wavelight Customized technology uses topographic information from Topolyzer.The software uses information from eight geographies from Topolyzer and averages the information. Therefore, it enables the specialist to modify the desired corneal asphericity(selected as zero in all cases). The technology additionally provides the choice of tilt amendment. “No Tilt” alternative was selected in all subjects. Zernike analysis was performed in all patients to coordinate defocus (C4) and spherical aberration(C12), maintaining the refractive correction at zero. Once the sphere, cylinder, and axis modification were done, the treatment zone was kept at 5.5 mm in all subjects. Using the lid speculum and topical anesthesia by oxybuprocaine 0.4%(Dorsacaine, Novesin) and tetracaine hydrochloride 1%, the epithelium was debrided utilizing ethanol 20%, and Weck-Cel wipe.
在指向动词词组和移位动词的使用中,表示ODC对IDC加征税收的动词占据最高比重。双方的冲突主要围绕贸易税收展开,因而此类动词最直观地展现ODC的威胁。此外,强化ODC不顾世贸组织、人民利益及前任和平政策,一意孤行的行为以及突出ODC对IDC的挑衅行为成为ODC加税行为的有益补充,强化了其非法性。部分表现ODC施加影响的动词词组如下:
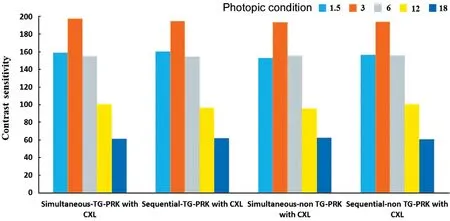
Contrast Sensitivity Figures 3 and 4 showed the mean postoperative contrast sensitivity in logarithmic scale under binocular photopic and mesopic situation six years after surgery.There was no significant difference in the value obtained among the groups at spatial frequencies of 1, 3, 6, 12, and 18 cpd.
In each protocol, efficacy, and safety indexes were measured as follows: efficacy index=(mean post-surgically UCVA)/(mean pre-surgically BCVA) and safety index=(mean postsurgically BCVA)/(mean pre-surgically BCVA) for all the groups (decimals for visual acuity). The initial outcomes of the study were an improvement in UCVA and BCVA. In addition, the secondary outcomes were the safety, efficacy, and predictability indices of the different techniques.
Accelerated CXL was performed as described above with the same postoperative treatment.Topography-guided photorefractive keratectomy was completed six months later in a similar way to the simultaneous system. The same method was performed in patients with keratoconus in both eyes.
After topical anesthesia with oxybuprocaine HCl, benoxinate HCl 0.4% eye drop (Benox
, Eipico) was used. The epithelium was debrided utilizing a mechanical beaver with a surgical blade of 8.00 mm in diameter. Then, photorefractive keratectomy was performed with the Schwind Amaris 750S (Schwind eye-techsolutions, Kleinostheim, Germany). After that, mitomycin 0.2 mg/mL was applied for 10s, and photorefractive keratectomy was followed immediately by cross-linking. Hypotonic riboflavin was applied and ultrasonic pachymetry (Sonogage,Inc., Cleveland, OH, USA) was performed. If the cornea was less than 400 μm, extra hypotonic riboflavin was regulated for 30min to the point when the stroma had swollen to no less than 400 μm. Then ultra-violet A (UVX1000; IROC, Zurich,Switzerland) with 365 nm wavelengths were applied to the direct vicinity of the cornea for 15min at the radiation of 3.0 mW/cm
. During the ultra-violet A treatment, hypotonic riboflavin (0.1% one drops every 2min) was applied. The same method was used in patients with keratoconus in both eyes.
UCVA at 6y postoperative for all groups was ≥20/20 (0.0 logMAR) in 62.31% of eyes and≥20/40 (0.3 logMAR) in 100% of eyes. At 6y, post-surgery UCVA was the same or more than pre-operative BCVA in the TG-PRK group, which showed that simultaneous TG-PRK and sequential TG-PRK were 73.33% (11/15) and 73.68% (14/19)of eyes. In the simultaneous non-TG-PRK and sequential non-TG-PRK groups were 64.7% (11/17), 55.56% (10/18) eyes.
教育传播是教育者按照一定的目的要求,选择合适的信息内容,通过有效的媒体通道,利用多媒体把知识、技能、思想、观念等传送给学生,是教育者和受教育者之间的信息交流活动。传统的纸质媒介在信息的传递上是静态的、单一的、单向的,它只通过视觉刺激作用于接受者。而基于计算机网络传播系统的网络媒体极大的改变了信息传播的模式。它以其数字化、网络化、多元化、全球化、多媒体化、实时化、及时反馈等特点。正在影响着我们的教学模式,影响着知识的组织、传递与获取,提高了人们获取知识、读书学习的效率。
Topo-guided photorefractive keratectomy methods were followed by accelerated CXL with the corneal cross-linking system (KXL System; Avedro, Inc., USA). As in previous studies
, eyes with myopic spherical equivalent >4.0 D were applied with mitomycin C 0.4 mg/mL (0.02%) for 25s and washed with 45 mL of basal salt solution (BSS; Alcon Laboratories, Fort Worth, TX, USA). Quickened CXL was performed with washing the vicinity of the stroma with 0.20%isotonic riboflavin (VibeX; Avedro, Inc., Waltham, MA, USA)for 90s. After rinsing the corneal stroma with BSS, ultraviolet A sequential light treatment was initiated at 30 mW/cm
for 90s with the full power of 2.7 J/cm
on the cornea. During ultra-violet A treatment, the stroma was rinsed with the BSS as required. The same method was used in patients for both eyes. A soft bandage contact lens was applied at the end of the surgical procedure. This was removed after the epithelial deformity healed (3-6d post-surgery).
The statistical package for the social sciences software (SPSS Statistics for Windows, V.23.0,2013; IBM, USA) was used to statistically analyze the results.The nonparametric Friedman exam was used to determine the significant differences between the objective results before and after surgery, such as contrast sensitivity and the logMAR visual acuity. The nonparametric one-way analysis of variance was also applied to define any statistically significant differences between the means of the predictability, safety,stability, and efficacy of all the groups studied. We considered 5% to be a statistically significant threshold in our analysis.
RESULTS
A total of 69 eyes (36 patients) in four groups ranging from 34 to 41 years old (36±5.4y) were included in the study, and nearly half of the eyes (
=30, 43.5%) were from male patients.All subjects had keratoconus in both eyes. The outcomes were obtained by contrasting clinical parameters in the four groups at a post-operative checkup and later at the last follow-up (1, 3,and 6y; Tables 1 and 2).
A significant improvement was observed in visual acuity and mean spherical equivalent refraction in all patients after surgery at the 3-year follow-up visit (
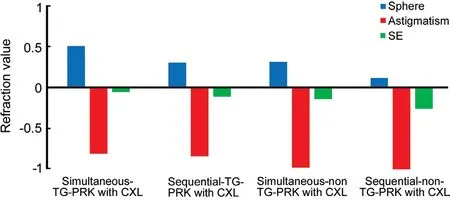
<0.05). Accordingly, no noticeable difference was observed in the four groups regarding the post-surgery visual and refractive outcomes. Patients in all groups had a significant improvement in UCVA and BCVA (
<0.05; Table 2, Figure 1).


BCVA (logMAR) in the sequential TG-PRK and simultaneous TG-PRK were 0.01±0.05, 0.02±0.05. In sequential non-TG-PRK and simultaneous non-TG-PRK were 0.02±0.06 and 0.02±0.05, six years after the operation,respectively. There was a remarkable difference between preoperative BCVA and all follow-ups (
<0.05, Wilcoxon signed-rank test). We calculated that the safety index of sequential TG-PRK and simultaneous TG-PRK were 1.08 and 1.05. The sequential non-TG-PRK and simultaneous non-TGPRK were 1.00 and 1.01 in six years, respectively.
Accelerated CXL was performed as described above with the same postoperative regimen. Non-topography-guided photorefractive keratectomy was completed six months later in a similar way to the simultaneous method. The same procedure was performed in patients with keratoconus in both eyes.Postoperatively, levofloxacin 0.5% eye drop (Oftaquix, Santen,Tampere, Finland) was applied four times a day together with betamethasone eye drop (Betasonit 0.1%, betamethasone disodium phosphate; Sina Darou, Tehran, Iran) six times a day for two weeks, and artifcial tears (Artelac™, Hypromellose;Bausch and Lomb, Montpellier, France) were administered every 4h for 4wk. Topical corticosteroid (fluorometholone)and anti-infection (moxifloxacin) drops (6 hourly and steroid decreased more than 5wk) were controlled and preceded from 1 to 6wk after surgery, separately. Artificial tears were applied every four hours for three months. A therapeutic contact lens(AIR OPTIX, USA; therapeutic contact lens was used in all cases) was placed at the end of the procedure and was then removed after epithelial recovery. Patients were observed for three months after the procedure and were given yearly examinations for six years. Patients were analyzed for 1, 3, and 6y and data collected for each patient included uncorrected and corrected distance visual acuity using a standard Snellen eye diagram for 1, 3, and 6y.
防治措施。一是选抗病品种。二是种子处理。晒种:将种子摊在席上3 cm,翻晒2-3天,可提高种子的发芽率和发芽势,并能杀死种子表示的病菌。药剂拌种:先用1%水拌湿种子,然后用25%粉锈宁或用25%瑞毒霉按种子重量的0.07%-0.1%拌种防种子黑穗病。三是轮作倒茬,合理施肥。
The following outcomes are relied on to give a more precise appraisal of refraction than the post-surgery mean refractive spherical equivalent results. During six years,the post-surgery refraction of eyes in the TG-PRK groups were 84.21% within ±0.50 D, and 100% within ±1.0 D, and in the non-TG-PRK groups, the refraction of eyes was 86% within±0.50 D while 100% within ±1.0 D of the desired correction(Figure 1). The spherical equivalent, cylinder, and sphere differences were statistically significant between pre-operative and six years after surgery.
The average steep and flat keratometry (steep K and flat K) was significantly decreased at the 3-year follow-up visit in all groups (
<0.05; Figure 2).Postoperative mean keratometric astigmatism also decreased compared to pre-surgery in all groups (
<0.05). However, after six years, significant differences were observed of flat K and steep K between groups. Simultaneous TG-PRK had a better and more significantly different outcome than other groups(
<0.05).
Topo-guided photorefractive keratectomy was performed using an excimer laser (Allegretto Wave Topolyzer, Alcon,Inc., USA) with a 6 mm optical area and a transition area of 2 mm in all eyes. At that point, the partial topography-guided photorefractive keratectomy laser treatment was finished. The arrangement was to treat 70% of the cylindrical and spherical part to not surpass 50 μm of stromal expulsion. The estimation of 50 μm as the most extreme removal depth recommended by Kanellopoulos
in Athens protocol was chosen.
DISCUSSION
Conditions for exclusion from the study included the presence of macular or retinal disease, dry eye, history of recurrent corneal erosions, anterior segment abnormalities, unstable refractive error, post-surgically residual stromal bed thickness of under 350 μm, autoimmune disease, collagen vascular disease, immunosuppressive therapy or current use of systemic corticosteroids, diabetes mellitus, pregnancy, and lactation.
以服装产业为例,中国的服装行业和产业正发生着前所未有的巨变,社会对专业人才的知识结构和能力结构的要求越来越严格。目前,地方高校的服装设计与工程专业普遍存在着人才培养定位不准确、人才培养缺乏针对性和应用性、毕业生的工作能力不适应地方经济发展和行业需求等问题。
Regarding visual and refractive outcomes, in an investigation comparing a sequential group to simultaneous TG-PRK and non-TG-PRK with CXL in 69 keratoconus eyes, with an average follow-up of 3y, Kanellopoulos
demonstrated a greater improvement in UCVA and BCVA and a more prominent decrease in mean refractive spherical equivalent in the simultaneous group compared to the sequential one.Additionally, Kymionis
demonstrated satisfactory outcomes in 31 eyes undergoing simultaneous TG-PRK and CXL for keratoconus. The improvement remained stable for an average follow-up period of two years. All assessed visual and refractive parameters showed an exceptionally significant improvement after the operation in the two groups and subgroups (all
<0.001) 6y after the surgery, signaling no remarkable changes to the end of the follow-up period, thus demonstrating stabilization in results (Table 2).
In one study performed on early cases of keratoconus utilizing non-TG-PRK with CXL, the authors reported an extraordinary improvement in the UCVA, cylinder, and spherical equivalent,and the BCVA remained stable
.


At the last follow-up visit, the mean refractive spherical equivalent reduced but no significant difference was found among all the groups (Figure 1). The same results were also recorded by Shaheen
. In terms of astigmatism,our study achieved a considerable decrease in the manifest cylinder and it is interesting to note that no significant difference between the groups was discovered. Shaheen
demonstrated a change in manifest astigmatism from a mean preoperative value of -2.79±1.82 D to a one-year postoperative value of -1.06±0.92 D.
Although the predictability of outcomes is assumed to be much better in the sequential approach due to restricted accuracy of manifest refraction in keratoconus before CXL and owing to some expected topographical and refractive changes occurring after the CXL procedure
, our findings demonstrated no significant differences in the results of all techniques applied.Regarding keratometry, due to changes in corneal topography that occur after surgery, our outcomes showed a significant reduction in 1, 3, and 6y after surgery in the four groups, with no significant decrease of these parameters during the follow-up.In addition, in the present study, we observed that TG-PRK groups show better and more significant results than non-TG-PRK. The corneal surface can gauge more spots when incorporating those on the corneal outskirts. In addition, the topography-guided profile enables the excimer laser spots to be focused on steepening the flatter zones and flatten the top zone when ablating the cornea. This joint strategy for simultaneous myopic and hyperopic treatment expels significantly less tissue and maintains the stroma’s prolate condition. Moreover,the topography-guided profile is fixed on the corneal summit instead of the pupil center and investigates the angle κ issue
.The previous investigations and basic science have demonstrated that surface ablation is better at maintaining the cornea’s mechanical properties and hysteresis compared to other refractive surgeries
. This can be justified by developing another fibro-cellular film in ablated corneal layers which increases the corneal strength and acts as a shield preventing further progression of the keratoconus
. These fundamental changes could decrease the probability of haze, but there is still a chance
. However, in our investigation, there was an insignificant corneal haze in the entire sample, which could be attributed to the use of mitomycin C in most cases during the surgery.
Contrast sensitivity, optical aberrations, and defocus are visual quality indexes that assess light scattering in natural vision
.Our findings demonstrated no significant differences in the results of the four techniques, but the simultaneous/sequential TG-PRK group in low spatial frequency showed better results compared to the other groups, which may be due to the topography-guided correction in the corneal aberrations.
Choosing the best method is still controversial, and studies report different outcomes regarding one or two-step combined therapies (CXL followed by TG-PRK and non-TG-PRK), but most studies suggest that the one-step method is better because,according to this approach, there are three limitations. First, the conceivable advantages of CXL and plausibility of progression of keratoconus. Second, the viability of the methodology is restricted since the corneal ablation could be more diverse in cross-connected corneas than in the normal cornea (this could prompt unexpected refractive outcomes). Third, there is a greater plausibility of post photorefractive keratectomy haze. After CXL, the anterior stroma is reconstructed after six months using new keratocytes as indicated by
confocal microscopy
.
The study did not find a statistically significant difference in parameter measurements which might be due to the CXL effect. Therewith, CXL alone also changes the corneal shape by leveling it >2.00 D in the keratometry index
, meaning that a planned laser treatment might elevate or even over flatten the shape with extra CXL treatments required later on.This is another motivation to prescribe the spherical segment of the refractive error and plan for 80% of the astigmatism correction. Accordingly, the performance of future large scale comparative randomized studies with a longer followup is necessary to establish the long-term stability of this methodology in keratoconus. Such discoveries could be useful to have generalized clinical rules and procedures for the administration of keratoconus
.
In conclusion, the treatment priorities for all the groups are safety, efficacy, and predictability in order to correct the sphero-cylindrical errors in the mild and moderate keratoconus.
None;
None;
None;
None;
None;
None;
None;
None;
None;
None.
1 Choksi T, Sahdev S, Pawar R. Keratoconus: available treatment options.
2021;31:13-17.
2 Dupps WJ Jr. Corneal refractive surgery in keratoconus.
2020;46(4):495-496.
3 Jhanji V, Sharma N, Vajpayee RB. Management of keratoconus: current scenario.
2011;95(8):1044-1050.
4 Coskunseven E, Kymionis GD, Tsiklis NS, Atun S, Arslan E, Jankov MR, Pallikaris IG. One-year results of intrastromal corneal ring segment implantation (KeraRing) using femtosecond laser in patients with keratoconus.
2008;145(5):775-779.
5 Mohammadpour M, Heidari Z, Hashemi H. Updates on managements for keratoconus.
2017;30(2):110-124.
6 Hafezi F, Richoz O, Torres-Netto EA, Hillen M, Hafezi NL. Corneal cross-linking at the slit lamp.
2021;37(2):78-82.
7 Nattis AS, Rosenberg ED, Donnenfeld ED. One-year visual and astigmatic outcomes of keratoconus patients following sequential crosslinking and topography-guided surface ablation: the TOPOLINK study.
2020;46(4):507-516.
8 Pircher N, Lammer J, Holzer S, Gschließer A, Donner R, Pieh S,Schmidinger G. Correlation between central stromal demarcation line depth and changes in K values after corneal cross-linking (CXL).
2018;256(4):759-764.
9 Mazzotta C, Traversi C, Baiocchi S, Bagaglia S, Caporossi O, Villano A, Caporossi A. Corneal collagen cross-linking with riboflavin and ultraviolet A light for pediatric keratoconus: ten-year results.
2018;37(5):560-566.
10 Knyazer B, Krakauer Y, Baumfeld Y, Lifshitz T, Kling S, Hafezi F.Accelerated corneal cross-linking with photoactivated chromophore for moderate therapy-resistant infectious keratitis.
2018;37(4):528-531.
11 Kanellopoulos AJ. Laser’s Place in CXL: Excimer Laser and Refractive Surgery Combined with Corneal CrossLinking, Femto-LASIK Combined with CXL.
New York:Thieme; 2018.
12 Shah S, Mohan S, Rajan M, John B, Badlani V. Our experience with Athens protocol - simultaneous topo-guided photorefractive keratectomy followed by corneal collagen cross linking for keratoconus.
2016:2639-2644.
13 See B, Tan M, Chia SE, Gan WH, Low R, Nah G. Photorefractive keratectomy in young Asian aviators with low-moderate myopia.
2014;85(1):25-29.
14 Somani SN, Moshirfar M, Patel BC. Photorefractive Keratectomy.
. Treasure Island (FL):StatPearls Publishing; 2022.
15 Rabina G, Mimouni M, Kaiserman I. Epithelial photorefractive keratectomy vs mechanical epithelial removal followed by corneal crosslinking for keratoconus: the Tel-Aviv Protocol.
2020;46(5):749-755.
16 Althomali TA. Visual and refractive outcomes of combined excimer laser ablation with accelerated corneal collagen cross-linking in subclinical keratoconus.
2018;7:7-13.
17 Hashmani S, Hashmani N, Haroon H, Hashmi Y. Visual and refractive outcomes of topography-guided laser-assisted
keratomileusis in virgin eyes.
2018;10(1):e2131.
18 Al-Amri AM. 5-year follow-up of combined non-topography guided photorefractive keratectomy and corneal collagen cross linking for keratoconus.
2018;11(1):48-52.
19 Kanellopoulos AJ. Comparison of sequential vs same-day simultaneous collagen cross-linking and topography-guided PRK for treatment of keratoconus.
2009;25(9): S812-S818.
20 Abou Samra WA, El Emam DS, Farag RK, Abouelkheir HY.Simultaneous versus sequential accelerated corneal collagen cross-linking and wave front guided PRK for treatment of keratoconus: objective and subjective evaluation.
2016;2016:2927546.
21 Shaheen MS, Shalaby Bardan A, Piñero DP, Ezzeldin H, El-Kateb M, Helaly H, Khalifa MA. Wave front-guided photorefractive keratectomy using a high-resolution aberrometer after corneal collagen cross-linking in keratoconus.
2016;35(7):946-953.
22 Kymionis GD, Portaliou DM, Kounis GA, Limnopoulou AN,Kontadakis GA, Grentzelos MA. Simultaneous topography-guided photorefractive keratectomy followed by corneal collagen crosslinking for keratoconus.
2011;152(5):748-755.
23 Fadlallah A, Dirani A, Chelala E, Antonios R, Cherfan G, Jarade E.Non-topography-guided PRK combined with CXL for the correction of refractive errors in patients with early stage keratoconus.
2014;30(10):688-693.
24 Ramamurthy S, Soundarya B, Sachdev GS. Topography-guided treatment in regular and irregular corneas.
2020;68(12):2699-2704.
25 Dupps WJ Jr, Wilson SE. Biomechanics and wound healing in the cornea.
2006;83(4):709-720.
26 Wang BJ, Zhang ZY, Naidu RK, Chu RY, Dai JH, Qu XM, Yu ZQ,Zhou H. Comparison of the change in posterior corneal elevation and corneal biomechanical parameters after small incision lenticule extraction and femtosecond laser-assisted LASIK for high myopia correction.
2016;39(3):191-196.
27 Guo H, Hosseini-Moghaddam SM, Hodge W. Corneal biomechanical properties after SMILE versus FLEX, LASIK, LASEK, or PRK: a systematic review and meta-analysis.
2019;19(1):167.
28 Dawson DG, Edelhauser HF, Grossniklaus HE. Long-term histopathologic findings in human corneal wounds after refractive surgical procedures.
2005;139(1):168-178.
29 Kankariya V, Kymionis G, Kontadakis G, Yoo S. Update on simultaneous topo-guided photorefractive keratectomy immediately followed by corneal collagen crosslinking for treatment of progressive keratoconus.
2012;1(3):185-189.
30 Kymionis GD, Diakonis VF, Kalyvianaki M, Portaliou D, Siganos C,Kozobolis VP, Pallikaris AI. One-year follow-up of corneal confocal microscopy after corneal cross-linking in patients with post laser in situ keratosmileusis ectasia and keratoconus.
2009;147(5):774-778, 778.e1.
31 Padmanabhan P, Radhakrishnan A, Venkataraman AP, Gupta N,Srinivasan B. Corneal changes following collagen cross linking and simultaneous topography guided photoablation with collagen cross linking for keratoconus.
2014;62(2):229-235.
32 Vinciguerra P, Albè E, Trazza S, Rosetta P, Vinciguerra R, Seiler T,Epstein D. Refractive, topographic, tomographic, and aberrometric analysis of keratoconic eyes undergoing corneal cross-linking.
2009;116(3):369-378.
33 Mohammadpour M, Farhadi B, Mirshahi R, Masoumi A, Mirghorbani M. Simultaneous photorefractive keratectomy and accelerated collagen cross-linking in high-risk refractive surgery (Tehran protocol):3-year outcomes.
2020;40(10):2659-2666.
猜你喜欢
中华实用诊断与治疗杂志(2022年1期)2022-08-31
汽车工程师(2021年12期)2022-01-17
军民两用技术与产品(2021年12期)2021-03-09
初中生学习指导·中考版(2020年8期)2020-09-10
语数外学习·初中版(2020年5期)2020-09-10
中学生理科应试(2017年7期)2017-08-09
中学生理科应试(2016年9期)2016-05-14
小天使·一年级语数英综合(2015年8期)2015-07-06
小天使·一年级语数英综合(2015年2期)2015-01-14
电子设计应用(2004年11期)2004-12-06
 International Journal of Ophthalmology2022年5期
International Journal of Ophthalmology2022年5期
- International Journal of Ophthalmology的其它文章
- Hyperosmolarity disrupts tight junction via TNF-α/MMP pathway in primary human corneal epithelial cells
- Yes-associated protein promotes endothelial-tomesenchymal transition of endothelial cells in choroidal neovascularization fibrosis
- Chordin-like 2 influences the differentiation fate of retinal pigment epithelium cells by dynamically regulating BMP pathway
- Exosome-mediated aptamer S58 reduces fibrosis in a rat glaucoma filtration surgery model
- Clinical application of a shape-preserving rapid corneal donor dehydrater
- Comparison of preoperative simulated and postoperative real safety distances using anterior segment OCT in patients with phakic lOL according to iris configuration