颅内动脉瘤破裂危险因素分析
2016-09-19 09:38赵志鸿高小平游伊伦
中风与神经疾病杂志 2016年7期
蒋 恒,赵志鸿,高小平,梁 辉,任 毅,张 欢,游伊伦,汪 洋,王 昕
颅内动脉瘤破裂危险因素分析
蒋恒,赵志鸿,高小平,梁辉,任毅,张欢,游伊伦,汪洋,王昕
目的探讨颅内动脉瘤破裂的危险因素。方法回顾分析2011年1月~2016年1月在我院确诊为颅内动脉瘤的373例患者的病历资料,根据动脉瘤破裂与否将研究对象分为破裂组(n=343)和未破裂组(n=30),对两组患者的临床资料及动脉瘤相关特征资料进行搜集,并进行单因素分析筛选,然后行Logistic回归分析。结果(1)经χ2分析及t检验示年龄、吸烟、饮酒、动脉瘤直径、动脉瘤部位等比较结果具有统计学意义(P<0.05)。(2)经logistic回归分析示颅内动脉瘤发生破裂的相关危险因素有青年(OR=1.437,95%CI=0.542~3.813)、老年(OR=1.083,95%CI=0.619~1.895)、中等动脉瘤(OR=1.764,95%CI=0.611~5.096)、前交通动脉瘤(OR=2.839,95%CI=1.238~6.509)、后交通动脉瘤(OR=1.102,95%CI=0.624~1.944)、高血压(OR=1.048 95%CI=0.585~1.877)、饮酒史(OR=1.286,95%CI=0.503~3.290)。结论青年、老年、高血压、饮酒史、中等动脉瘤、前交通动脉瘤、后交通动脉瘤是颅内动脉瘤破裂的相关危险因素。
颅内动脉瘤;破裂;危险因素
颅内动脉瘤(intracrania aneurysms,IA)是造成蛛网膜下腔出血的首要病因,具有高发病率、高致死率、高致残率的特点,对于未破裂颅内动脉瘤是否应该被治疗以防止未来的破裂存在着诸多争议[1,2],本文主要对颅内动脉瘤破裂相关危险因素进行探讨,以期为临床筛选出颅内动脉瘤破裂高风险人群提供参考。
1 资料和方法
1.1一般资料随机检索2011年1月~2016年1月于我院DSA确诊的373例颅内动脉瘤患者为研究对象,根据动脉瘤的破裂与否分为破裂组(n=343)和未破裂组(n=30)。破裂组男128例,女215例;年龄29~85岁,平均(56.7±11.0)岁。未破裂组男15例,女15例;年龄37~82岁,平均(66.9±12.7)岁。颅内动脉瘤破裂组纳入标准:临床资料准确完整;临床主要表现为颅神经损伤、颈项部及头部疼痛、意识障碍或颈项强直;经DSA检查后,确诊为由瘤体破裂导致的蛛网膜下腔出血。未破裂颅内动脉瘤组纳入标准:临床资料准确完整;无明显临床表现,经体检确定为未破裂颅内动脉瘤或具有头痛、颅神经损伤等临床表现;经DSA检查后确诊;从未发生过颅内动脉瘤破裂。排除标准:颅内动脉瘤为再次破裂并采取手术治疗。
1.2研究方法对性别、高血压、吸烟、饮酒、动脉瘤部位等定性资料采用χ2检验,年龄、动脉瘤数量、动脉瘤大小等等级资料采用独立样本t检验,P<0.05 为差异有统计学意义。并对上述各变量进行单因素方差分析筛选有意义的危险因素后进行logistic回归多因素分析,其中年龄分组:青年(≤44岁),中年(45~59岁),老年(≥60岁),动脉瘤直径分组:小动脉瘤(<5 mm),中等动脉瘤(5~10mm),大动脉瘤(11~25 mm),巨大动脉瘤(大于25 mm),相对危险度和可信区间分别用OR值和95%CI表示。
1.3统计学方法选用SPSS 22.0软件行统计学分析,两组临床资料及动脉瘤特征定性资料采用χ2检验,率或构成比以百分比表示,等级资料采用独立样本t检验,P<0.05表示差异有统计学意义。另通过单因素分析筛选危险因素后,采用Logistic回归多因素分析。
2 结 果
2.1临床资料两组患者的年龄(P<0.01)、吸烟史(P<0.01)、饮酒史(P<0.05)的差异有统计学意义。两组患者的性别、高血压、高血糖、高血脂差异无统计学意义(P>0.05)。见表1。
2.2动脉瘤特征本组373例,单发患者293例,多发患者80例,480个动脉瘤(包括多发患者)。其中大脑后动脉瘤及大脑前动脉瘤组中,大脑前动脉瘤破裂组为14个,未破裂组为8个,大脑后动脉瘤破裂组为1个,未破裂组为2个;小脑后下动脉瘤及小脑上动脉瘤组中,小脑后下动脉瘤破裂组为5个,未破裂组为0个,小脑上动脉瘤破裂组为1个,未破裂组为0个。两组患者的动脉瘤部位(P<0.01)、动脉瘤直径(P<0.01)差异有统计学意义,动脉瘤数量(P>0.05)差异无统计学意义。见表2。
2.3Logistic回归分析经单因素方差分析筛选危险因素之后,进行Logistic回归分析结果示青年、老年、中等动脉瘤、前交通动脉瘤、后交通动脉瘤、高血压、饮酒史是造成动脉瘤破裂的主要危险因素,青年患者较老年患者更易发生动脉瘤破裂,前交通动脉瘤较后交通动脉瘤更易破裂。见表3。

表1 2组临床资料比较[n(%)]

表2 破裂组与未破裂组颅内动脉瘤特征比较[n(%)]
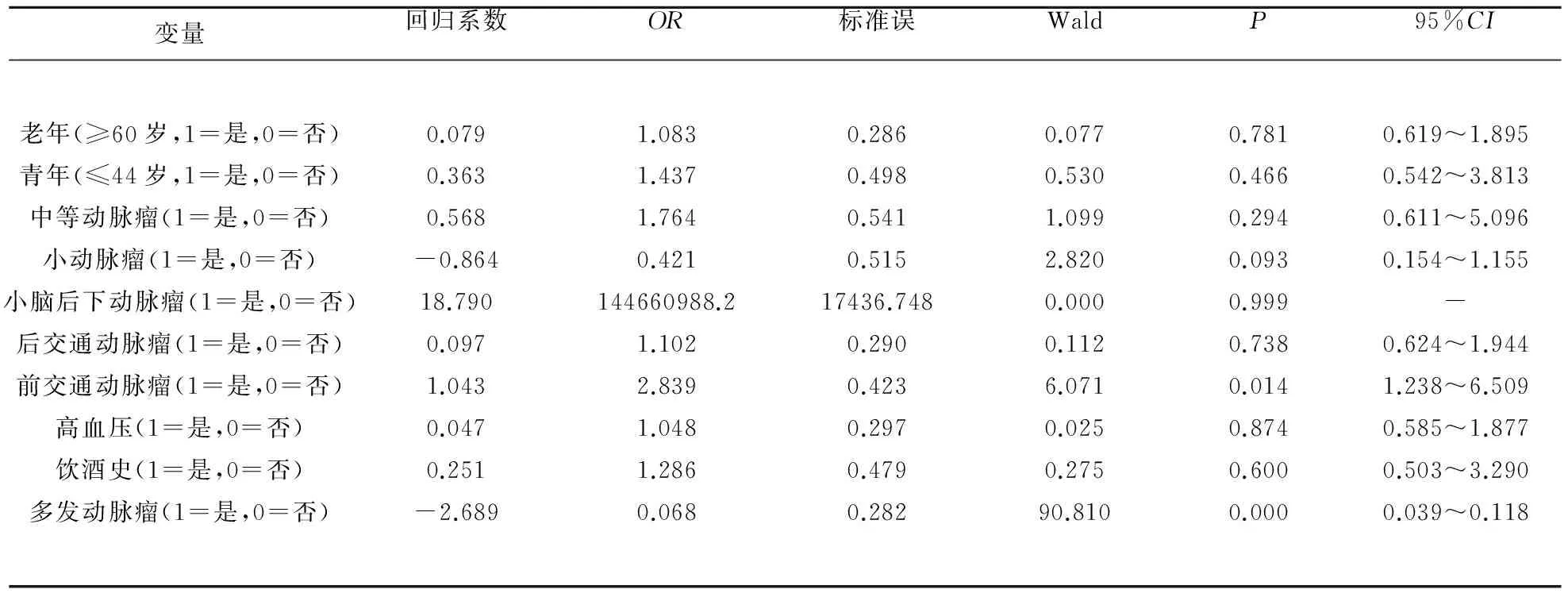
表3 颅内动脉瘤破裂相关危险因素Logistic回归分析结果
3 讨 论
在本研究中,我们通过临床资料及动脉瘤特征筛选动脉瘤破裂的危险因素,表明年龄、动脉瘤直径及位置、高血压、饮酒史为动脉瘤破裂的相关危险因素。
国外学者对于年龄尚存争议。有文献报道,低龄更易发生动脉瘤破裂[3~5],也有学者认为,随着年龄的增加,动脉瘤破裂的几率也会增大,而Wermer 等也以相关文献证实,年龄>60岁颅内动脉瘤患者具有更高的动脉瘤破裂几率[6~8],这可能与老年人动脉壁顺应性下降,而青年人更易发生情绪波动有关。对于不同年龄段颅内动脉破裂的风险还需进一步研究,而在本研究中,青年及老年均是危险因素,青年较老年更易发生动脉瘤破裂。
许多文献报道,颅内动脉瘤的破裂与高血压有关[5,7,9],然而也有一部分学者认为,高血压与颅内动脉瘤破裂的发生没有相关性[8,10,11],这可能与颅内动脉瘤患者的血压控制情况良好有关,目前普遍认为血压波动是颅内动脉瘤破裂的危险因素,而一过性血压升高更是颅内动脉瘤破裂的根本因素[12],本研究表明,高血压是颅内动脉瘤破裂的相关危险因素,另饮酒史也是危险因素之一,饮酒本身不会影响颅内动脉瘤的形成和生长[13],这可能与饮酒后血压波动有关。
有文献报道,颅内动脉瘤(>5 mm)破裂风险高于小动脉瘤(2~4 mm),椎基底动脉瘤及后交通动脉瘤是动脉瘤破裂的危险因素[14],日本的一项5722例患者的单中心大样本量的颅内动脉瘤研究报道,随着动脉瘤直径的增加,动脉瘤破裂的风险增大,且前交通动脉及后交通动脉更易破裂[15]。而有中国学者报道,90%的破裂动脉瘤大小在10 mm以下[16],还有学者报道,中国人中5 mm以下的颅内动脉瘤更容易破裂[17]。在本研究中,中等动脉瘤(5~10 mm)、前交通动脉及后交通动脉是颅内动脉瘤破裂的相关危险因素,且前交通动脉瘤较后交通动脉瘤更易破裂。
在本研究中老年及青年、饮酒史、高血压、中等动脉瘤、前交通动脉瘤、后交通动脉瘤是颅内动脉瘤破裂的相关危险因素,可为今后临床治疗抉择提供参考。本研究存在着一些不足之处,作为单中心,难免造成统计学的偏倚,样本含量也不够大,有待进一步完善。
[1]Etminan N,Beseoglu K,Barrow DL,et al. Multidisciplinary consensus on assessment of unruptured intracranial aneurysms:proposal of an international research group[J]. Stroke,2014,45:1523-1530.
[2]Ishibashi T,Murayama Y,Saguchi T,et al. Justification of unruptured intracranial aneurysm repair:a single-center experience[J]. AJNR Am J Neuroradiol,2013,34:1600-1605.
[3]White PM,Wardlaw JM,Easton V. Can noninvasive imaging accurately depict intracranial aneurysms? A systematic review[J]. Radiology,2000,217(2):361-370.
[4]Juvela S,Poussa K,Lehto H,et al. Natural history of unruptured intracranial aneurysms:a long-term follow-up study[J]. Stroke,2013,44:2414-2421.
[5]Sonobe M,Yamazaki T,Yonekura M,et al. Small unruptured intracranial aneurysm verifi cation study:SUAVe study,Japan[J]. Stroke,2010,41:1969-1977.
[6]Vlak MH,Rinkel GJ,Greebe P,et al. Trigger factors for rupture of intracranial aneurysms in relation to patient and aneurysm characteristics[J]. Neurol,2012,259:1298-1302.
[7]Williams LN,Brown RD Jr. Management of unruptured intracranial aneurysms[J]. Neurol Clin Prac,2013,3:99-108.
[8]Juvela S,Porras M,Poussa K. Natural history of unruptured intracranial aneurysms:probability of and risk factors for aneurysm rupture[J]. J Neuros,2008,108:1052-1060.
[9]Steiner T,Juvela S,Unterberg A,et al. European Stroke Organization guidelines for the management of intracranial aneurysms and subarachnoid haemorrhage[J]. Cerebrovasc Dis,2013,35:93-112.
[10]Inagawa T. Risk factors for the formation and rupture of intracranial saccular aneurysms in Shimane,Japan[J]. World Neurosurgery,2010,73:155-164.
[11]Vlak MH,Rinkel GJ,Greebe P,et al. Risk of rupture of an intracranial aneurysm based on patient characteristics:a case-control study[J]. Stroke,2013,44:1256-1259.
[12]Suarez JI,Tarr RWS,Selman WR. Aneurysmal subarachnoid hemorrhage[J]. N Engl J Med,2006,354(4):387-396.
[13]Chalouhi N,Chitale R,Jabbour P,et al. The case for family screening for intracranial aneurysms[J],Neurosurg Focus,2011,31(6):E8.
[14]Murayama Y,Takao H,Ishibashi T,et al. Risk analysis of unruptured intracranial aneurysms:prospective 10-year cohort study[J]. Stroke,2016,47:365-371.
[15]Morita A,Kirino T,Hashi K,et al. The natural course of unruptured cerebral aneurysms in a Japanese cohort[J]. New England J Med,2012,366:2474-2482.
[16]Zhao L,Zhang L,Zhang X,et al. An analysis of 1256 cases of sporadic ruptured cerebral aneurysm in a single chinese institution[J]. PloS one,2014,9:e85668.
[17]Yu SC,Chan MS,Boel R,et al. Intracranial aneurysms treated with Guglielmi detachable coils:midterm clinical and radiological outcome in 97 consecutive Chinese patients in Hong Kong[J]. Am J Neuroradiol,2004,25:307-313.
Study on risk factors of intracranial aneurysm rupture
JIANGHeng,ZHAOZhihong,GAOXiaoping,etal.
(DepartmentofNeurology,HunanProvincialPeople’sHospital,Changsha410005,China)
ObjectiveTo explore the risk factors of the ruptured intracranial aneurysm. MethodsRetrospectively analysis 373 cases which were diagnosed with intracranial aneurysm in our hospital during 2011 Jan-2016 Jan. According to the rupture of aneurysm,subjects were divided into ruptured group(n=343) and unruptured group(n=30). The clinic data and aneurysm related features were collected and brought into the univariate linear regression analysis,which were filtered with Binary Logistic regression afterwards. Results(1)chi square analysist-test showed that age,smoking,drinking,aneurysm diameter,aneurysm location comparison results with statistical significance (P<0.05). (2)Binary Logistic regression revealed that the related risk factors of intracranial aneurysm rupture including youth(OR=1.437,95%CI=0.542~3.813),gerontism(OR=1.083,95%CI=0.619~1.895),Medium aneurysm(OR=1.764,95%CI=0.611~5.096),Anterior communicating artery aneurysm(OR=2.839,95%CI=1.238~6.509),posterior communicating artery aneurysm(OR=1.102,95%CI=0.624~1.944),Hypertension(OR=1.048 95%CI=0.585~1.877),History of alcohol(OR=1.286,95%CI=0.503~3.290). ConclusionThe related risk factors of intracranial aneurysm rupture include youth,gerontism,hypertension,history of alcohol,Medium aneurysm,anterior communicating artery aneurysm and posterior communicating artery aneurysm.
Intracranial aneurysm;Rupture;Risk factors
1003-2754(2016)07-0625-04
2016-01-20;
2016-06-22
湖南省科技厅资助项目(No. 2013FJ3119)
(湖南省人民医院神经内科,湖南 长沙 410005)
赵志鸿,E-mail:1019200187@qq.com
R739.41
A
猜你喜欢
童话世界(2020年32期)2020-12-25
中国生殖健康(2019年5期)2019-01-06
小学生导刊(2018年16期)2018-07-02
小小艺术家(2018年1期)2018-06-05
中华诗词(2017年5期)2017-11-08
Coco薇(2016年8期)2016-10-09
新少年(2015年6期)2015-06-16
海外英语(2013年11期)2014-02-11
中学英语之友·上(2008年1期)2008-03-20