
全髋关节置换术后早期负重可行性的研究进展
2018-06-22 05:48汪鑫杨延砚周谋望徐珑
中国骨与关节杂志 2018年6期
汪鑫 杨延砚 周谋望 徐珑
20 世纪 60 年代,全髋关节置换术 ( total hip arthroplasty,THA ) 开始在临床上应用,经过半个世纪的发展,已成为治疗髋关节疾病,重建关节功能最有效的手术[1]。手术中所需假体材料和外科方法不断发展进步,而相关围手术期康复也随之不断跟进。现就 THA 术后早期负重问题综述如下,以期为临床实践提供参考。
一、THA 手术假体的应用历史
全髋关节植入组合通常由惰性金属 ( 钴铬合金和钛 )的股骨组件和一个高密度的聚乙烯髋臼组成[2]。早期 THA手术的革命性进展是使用丙烯酸的骨水泥固定假体。骨水泥固定术后允许早期负重,有效缩短患者住院天数,但由于骨水泥植入物,特别是髋臼假体常出现机械松动,从而促进了非骨水泥固定的发展[3]。非骨水泥固定,通过使用多孔涂层假体以及近年发展的压配技术,使骨成串珠状或网格状长入表面植入物,同时,生物活性涂层假体的运用促进了骨的长入[4]。
二、THA 术后早期负重的争议
THA 两种固定方式的适应证:骨水泥固定主要适用于患有骨质疏松症的老年患者。非骨水泥固定主要适用于参加运动较多,60 岁以下骨质良好的患者[5]。术后最初几个星期,假体固定类型可能会影响患者的负重和功能活动[6]。研究表明如果 THA 术后允许早期完全负重,患者功能康复更容易实现[7-8]。但非骨水泥固定 THA 术后早期负重仍存在争议,有人认为为防止股骨干假体下沉和骨质流失,术后至少持续 6 周进行保护下负重和活动限制[9]。但是,近年的文献证实,非骨水泥固定 THA 术后早期负重对假体稳定性没有不利影响[10-13]。
三、THA 术后早期负重的可行性
目前,对于骨水泥型 THA 术后,允许患者在可能耐受的负荷范围内早期负重已经形成共识。虽然许多骨科医师在非骨水泥和混合型 THA 术后限制负重,但这种做法随着紧密压配型假体的使用越来越受到质疑。限制负重是基于这样的假设,即术后早期过度的负荷会导致假体与骨面的微动,影响植入假体的稳定,干扰骨生成,最终使得假体松动甚至脱落[14-15]。但是由于术后早期限制负重,卧床时间相应延长,使得并发症发生率增高[16],另外继发性的骨质疏松影响假体稳定,导致假体松动[17]。有文献报道,如果术中可使假体在良好位置下紧密固定,术后早期负重不会影响假体的稳定性以及患者功能的恢复[8,18]。另外,在安全范围内进行早期负重也有潜在的好处,特别是减少因减少负重引起的骨质流失以及促进功能活动的早期恢复[19-20]。需要注意的是,许多患者在日常训练中不能有效地控制负重程度,经常使患侧下肢承受超过规定的负荷[21-23]。此外,在仰卧位下下肢持续活动所受的负荷远大于体重[24]。鉴于这些考虑,非骨水泥 THA 术后限制负重的需要值得研究。不仅如此,非骨水泥固定或混合型固定THA 术后负重的程度受许多因素的影响[7,25]( 表1 )。

表1 THA 术后早期负重的限制因素Tab.1 Limiting factors of early load-bearing after THA
1. 对假体稳定性的影响:瑞士 Wolf 等[26]的研究中,37 例单侧髋关节置换术后的患者,分成术后完全负重和部分负重两组,随访 5 年,通过放射立体测量 ( radio stereometric analysis,RSA ) 评估。RSA 作为非侵害性手段评估假体稳定的金标准,已经广泛用于 THA 术后假体稳定性的评定。术后立即完全负重,引起较多的向心偏移和倾斜度的增加,但是数值并未超过精密度的限制范围。整合两组数据,显示 5 年中有 0.1~0.3 mm 的偏移和 0.2°~0.3° 的旋转。通过 5 年随访结果,证实术后早期负重协同一定强度的康复计划对紧密压配型 THA 假体的稳定性没有不利影响。
另外,Thien 等[18]将 43 例因单侧髋关节骨关节炎接受非骨水泥固定羟基磷灰石涂层假体置换的患者,患者随机分为术后 6 周内部分负重 ( P 组 ) 和完全负重 ( F 组 )两组。研究中使用 RSA 进行评估。随访 3 个月,P 组和F 组假体平均近端 ( + ) / 远端 ( - ) 移动分别为 -0.14 mm( -1.93~0.11 ) 和 -0.31 mm ( -4.30~0.16 )。随访 1 年,平均移动数值分别为 -0.17 mm ( -2.18~0.21 ) 和 -0.28 mm( -4.31~0.11 )。两组假体干旋转程度无明显不同。两组的髋臼移动、旋转和股骨头嵌入程度相似。结论是:非骨水泥 THA 术后早期负重有效可行,没有不良反应。
2. 对骨密度的影响:Wolf 等[27]就非骨水泥术后不同负重对骨密度和身体成分影响进行研究。29 例随机分为术后早期负重和部分负重 3 个月两组。采用双能 X 线吸收测量法测量对侧髋关节、两侧足跟骨密度以及体成分。术后 3 个月和 12 个月,不同负重方式对骨密度和体成分的变化没有影响。术后 5 年,全身总共减少 3% 的骨密度,在对侧髋关节区域为 2%~3%,并且发现全身骨矿物质减少了 5% 的含量,但是比起术前脂肪和肌肉组织质量没有变化。因此,他们认为术后负重方式对体成分和骨矿物质密度没有影响。
3. 对髋关节功能的影响:另外有研究探讨非骨水泥THA 术后负重的安全性。Bernasek 等[19]研究将 329 例行非骨水泥 THA 患者分两组,一组术后开始保护下负重行走 6 周,另一组术后开始完全负重行走。随访 6 个月。通过 Harris 髋关节量表和 X 线片评估,相关并发症、疼痛及再入院原因无差异,影像学诊断数据差异也没有达到相关标准。置换术后所有患者诊断结果良好,X 线片中所有股骨干稳定。
此外,Markmiller 等[28]将 100 例 HA 涂层假体 THA患者分部分负重和完全负重两组,在术后 6 周内,部分负重组术后立即开始 15 kg 负重,完全负重组术后开始完全负重行走。实验前后使用 Merle d’Aubigne 髋关节评分,视觉疼痛模拟评分 ( visual analogue scale,VAS ) 以及 X 线测量来进行比对。术后 3 个月和 24 个月的随访结果显示,两组髋关节评分差异无统计学意义,也没有任何病例进一步发生>1 mm 轴移,无 5 mm 以上的偏移 以及股骨干的下沉。影像学诊断明确了所有的股骨假体固定良好,骨组织的正常生长。
这意味着假体干的稳定性独立于手术后不同负重机制。非骨水泥股骨假体的稳定性是由髓腔和假体柄手术中的契合和随后骨在羟基磷灰石涂层假体的植入程度决定[29]。因此患者可以在 HA 涂层假体 THA 术后完全负重的情况下安全的步行 ( 表2 )。
以上研究证实,THA 术后早期完全负重锻炼是有效可行的,不会影响假体的稳定性以及患者髋关节的功能恢复。而且相关文献证实老年患者接受非骨水泥型 THA 与接受骨水泥型 THA 一样,可以进行术后早期负重[30-31]。当然早期康复治疗要个体化,并非所有患者均能早期负重[32]。应该充分考虑患者的年龄、术后全身状况以及是否有出现感染、假体早期脱位、血管神经损伤等并发症;植入假体初始稳定性不佳,包括术中进行截骨、植骨、骨裂或骨折,假体安放不正确,各种原因导致术后髋周软组织严重不平衡,以及术后的肌力和关节活动度情况,术后翻修手术等[7,33]。对不适合的患者仍要按照骨科常规处理,延迟负重以及进行相应的康复治疗。
四、THA 术后负重练习方法
全髋置换术后的康复治疗很大程度上影响着肢体功能的恢复[30,34]。术后训练不仅加强髋关节周围的肌力,而且使关节更加稳定,更有助于步态正常化[35-36]。检验术后康复训练最有效的措施便是有效恢复患者独立进行日常生活和工作的能力[37]。康复训练应个体化,在确定个体化训练方案时,应考虑手术方式,术后处理和可能的并发症[8,38]。
THA 负重训练包括从肌力训练开始的基础康复训练和负重训练[39]。基础康复训练分为肌力训练、关节活动训练、体位管理及训练等;负重训练包括基本的重心转移练习和行走练习[40]。
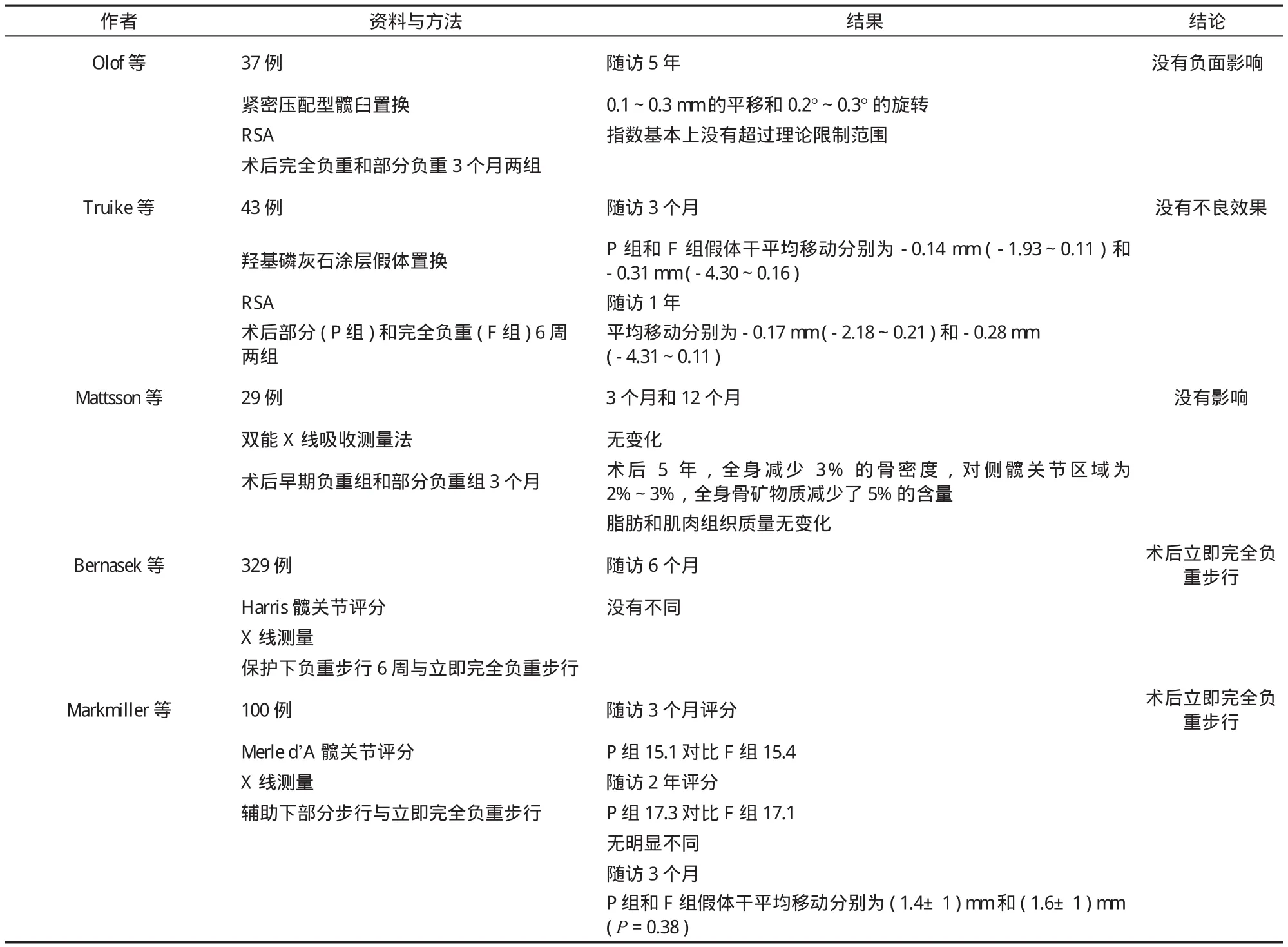
表2 非骨水泥固定 THA 术后立即完全负重的研究Tab.2 Immediate full load-bearing of non-cement fi xed THA
1. 基础练习:有调查研究显示,在各阶段的康复目标中,应重点练习的肌肉分别为髋外展肌 ( 62.2% ),其次是股四头肌 ( 16.9% ) 和其它的肌肉 ( 21% )[41-42]。运动练习侧重点包括负重 ( 42% )、功能 ( 45% ) 和体位 ( 13% )。
术前应指导患者进行肌肉收缩锻炼,使患肢肌力在术前有所恢复。康复训练强调臀中肌力量练习,臀中肌是否恢复到理想力量决定了术后功能恢复程度。它提供了躯干和骨盆的外侧稳定,因此在步态的单腿支撑期是维持平衡的关键[43-44]。
关节活动训练关节运动训练应遵循由被动到主动、逐渐加大关节活动范围、循序渐进、缓慢进行的原则[45],包括踝关节背屈跖屈运动、髌骨推移运动、仰卧位屈髋屈膝运动 ( 可用 CPM 进行 ) 等。
体位管理及训练仰卧位时保持患肢外展中立位,腿间放一软枕,保持患肢外展 ≥ 30°,防止因内收内旋、过伸外旋造成的后、前脱位;在进行仰卧位到侧卧位训练时,注意保护患侧,将患肢与身体同时由平卧转为侧卧,并在两腿间垫上枕头保持患肢外展位,禁止内收内旋;当进行仰卧位到坐位训练时,患者双手支撑坐起,屈健腿伸患腿,利用双手和健侧腿将患肢移至床缘,小腿自然垂于床边。
2. 负重练习:在进行重心转移训练时,帮助患者扶拐站好,指导患者双足分开与肩同宽,身体重心放在健肢,患肢伸直,然后将身体重心缓慢向患肢转移。
进行步态训练时,患肢必须先以足跟着地,然后将重心移至前脚掌。双足着地时间应相等,以免造成跛行。指导患者正确转移重心,调整步态,根据耐受情况安排训练时间和强度[46]。
3. 强化练习:这类练习旨在加强锻炼髋部肌肉,多采用临床实践中常用的练习。在之前练习的基础上,该阶段的强化练习有助于缓解疼痛和进一步提高肢 体功能。这些练习旨在加强股四头肌、绳肌、髋外展肌力,改善平衡功能[47]。训练程度由患者重复完成 10 次给定动作的能力决定 ( 表3 )。
综上所述,在术中假体契合稳定以及排除相应限制因素的前提下,THA 术后立即进行完全负重是安全可行的,不但不会对髋关节功能、假体的稳定和骨密度产生不利影响,还能有效提高 THA 术后的恢复效果、减少并发症及缩短住院时间。

表3 髋关节功能训练Tab.3 Hip function training
[1] Mellon SJ, Liddle AD, Pandit H. Hip replacement: landmark surgery in modernmedical history[J]. Maturitas, 2013,75(3):221-226.
[2] Hol AM, van Grinsven S, Lucas C, et al. Partial versus unrestricted weight bearing after an uncemented femoral stem in total hip arthroplasty: recommendation of a concise rehabilitation protocol from a systematic review of the literature[J]. Arch Orthop Trauma Surg, 2010, 130(4):547-555.[3] Jerosch J, Heisel J. Konzept Perioperative management for endoprosthetic hip joint replacement. The functional interdisciplinary therapy (FIT) concept[J]. Unfallchirurg, 2010,113(1):6-13.
[4] Cochu G, Mabit C, Gougam T, et al. Total hip arthroplasty for treatment of acute acetabular fracture in elderly patients[J]. Rev Chir Orthop Reparatrice Appar Mot, 2007, 93(8):818-827.
[5] Bergmann G, Bender A, Dymke J, et al. Standardized loads acting in hip implants[J]. PLoS One, 2016, 19;11(5):e0155612.
[6] Dickstein R, Yoeli Y, Holtzman S, et al. Weight bearing on the affected lower limb in residents of a geriatric rehabilitation hospital[J]. Am J Phys Med Rehabil, 2010, 89(4):287-292.
[7] Murphy CG, Carrothers AD. Fix and replace; an emerging paradigm for treating acetabular fractures[J]. Clin Cases Miner Bone Metab, 2016, 13(3):228-233.
[8] Eulenburg C, Rahlf AL, Kutasow A, et al. Agreements and disagreements in exercise therapy prescriptions after hip replacement among rehabilitation professionals: a multicenter survey[J]. BMC Musculoskelet Disord, 2015, 16:185.
[9] Tsukagoshi R, Tateuchi H, Fukumoto Y, et al. Functional performance of female patients more than 6 months after total hip arthroplasty shows greater improvement with weightbearing exercise than with non-weight-bearing exercise.Randomized controlled trial[J]. Eur J Phys Rehabil Med, 2014,50(6):665-675.
[10] Ng FY, Zhu Y, Chiu KY. Cementless acetabular component inserted without screws-the effect of immediate weightbearing[J]. Int Orthop, 2007, 31(3):293-296.
[11] Merle J, Rougier P, Belaid D, et al. Is early weight bearing resumption beneficial after total hip replacement[J]? Orthop Traumatol Surg Res, 2009, 95(2):127-133.
[12] Taunt CJ Jr, Finn H, Baumann P. Immediate weight bearing after cementless total hip arthroplasty[J]. Orthopedics, 2008,31(3):223.
[13] Tian P, Li ZJ, Xu GJ, et al. Partial versus early full weight bearing after uncemented total hip arthroplasty: a metaanalysis[J]. J Orthop Surg Res, 2017, 12(1):31.
[14] Bhargava P, Shrivastava P, Nagariya S. Assessment of changes in gait parameters and vertical ground reaction forces after total hip arthroplasty[J]. Indian J Orthop, 2007, 41(2):158-162.
[15] Wesseling M, Meyer C, Corten K, et al. Does surgical approach or prosthesis type affect hip joint loading one year after surgery[J]? Gait Posture, 2016, 44:74-82.
[16] Ström H, Nilsson O, Milbrink J, et al. The effect of early weight bearing on migration pattern of the uncemented CLS stem in total hip arthroplasty[J]. J Arthroplasty, 2007, 22(8):1122-1129.[17] Goebel S, Steinert AF, Schillinger J, et al. Reduced postoperative pain in total hip arthroplasty after minimal-invasive anterior approach[J]. Int Orthop, 2012, 36(3):491-498.
[18] Thien TM, Ahnfelt L, Eriksson M, et al. Immediate weightbearing after uncemented total hip arthroplasty with an anteverted stem: aprospective randomized comparison using radiostereometry[J]. Acta Orthop, 2007, 78(6):730-738.
[19] Bernasek TL, Thatimatla NK, Levering M, et al. Effect of immediate full weight bearing on abductor repair and clinical function after THA through a modifi ed Hardinge approach[J].Orthopedics, 2013, 36(3):e266-270.
[20] Siebens HC, Sharkey P, Aronow HU, et al. Outcomes and weight-bearing status during rehabilitation after arthroplasty for hip fractures[J]. PMR, 2012, 4(8):548-555.
[21] Hurkmans HL, Bussmann JB, Benda E, et al. Effectiveness of audio feedback for partial weight-bearing in and outside the hospital: a randomized controlled trial[J]. Arch Phys Med Rehabil, 2012, 93(4):565-570.
[22] Hurkmans HL, Bussmann JB, Benda E. Validity and interobserver reliability of visual observation to assess partial weightbearing[J]. Arch Phys Med Rehabil, 2009, 90(2):309-313.
[23] Schaefer A, Hotfi el T, Pauser J, et al. Incompliance of total hip arthroplasty (THA) patients to limited weight bearing[J]. Arch Orthop Trauma Surg, 2015, 135(2):265-269.
[24] Jauch SY, Huber G, Sellenschloh K, et al. Micromotions at the taper interface between stem and neck adapter of a bimodular hip prosthesis during activities of daily living[J]. J Orthop Res,2013, 31(8):1165-1171.
[25] Glaser D, Dennis DA, Komistek RD, et al. In vivo comparison of hip mechanics for minimally invasive versus traditional total hip arthroplasty[J]. Clin Biomech (Bristol, Avon), 2008,23(2):127-134.
[26] Wolf O, Mattsson P, Milbrink J, et al. Effects of postoperative weight-bearing on body composition and bone mineral density after uncemented total hip arthroplasty[J]. J Rehabil Med,2013, 45(5):498-503.
[27] Wolf O, Mattsson P, Milbrink J, et al. The effects of different weight-bearing regimes on press-fi t cup stability: a randomised study with five years of follow-up using radiostereometry[J].Int Orthop, 2012, 36(4):735-740.
[28] Markmiller M, Weiss T, Kreuz P, et al. Partial weightbearing is not necessary after cementless total hip arthroplasty: a two-year prospective randomized study on 100 patients[J]. Int Orthop,2011, 35(8):1139-1143.
[29] Karatosun V, Unver B, Gunal I. Hip arthroplasty with the thrust plateprosthesis in patients of 65 years of age or older:67 patients followed 2-7 years[J]. Arch Orthop Trauma Surg,2008, 128(4):377-381.
[30] Resch H, Krappinger D, Moroder P, et al. Treatment of acetabular fractures in older patients-introduction of a new implant for primary total hip arthroplasty[J]. Arch Orthop Trauma Surg, 2017, 137(4):549-556.
[31] Rutz E, Leumann A, Rutz D, et al. Total hip arthroplasty for fractures of the proximal femur in older patients[J]. Hip Int,2010, 20(2):215-200.
[32] Dolata J, Pietrzak K, Manikowski W, et al. Infl uence of age on the outcome of rehabilitation after total hip replacement[J]. Pol Orthop Traumatol, 2013, 78:109-113.
[33] Umpierres CS, Ribeiro TA, Marchisio ÂE, et al. Rehabilitation following total hip arthroplasty evaluation over short followup time: randomized clinical trial[J]. J Rehabil Res Dev, 2014,51(10):1567-1578.
[34] Monticone M, Ambrosini E, Rocca B, et al. Task-oriented exercises and early full weight-bearing contribute to improving disability after total hip replacement: a randomized controlled trial[J]. Clin Rehabil, 2014, 28(7):658-668.
[35] Di Monaco M, Vallero F, Tappero R, et al. Rehabilitation after total hip arthroplasty: a systematic review of controlled trials on physical exercise programs[J]. Eur J Phys Rehabil Med,2009, 45(3):303-317.
[36] Coulter CL, Scarvell JM, Neeman TM, et al. Physiotherapistdirected rehabilitation exercises in the outpatient or home setting improve strength, gait speed and cadence after elective total hip replacement: a systematic review[J]. J Physiother,2013, 59(4):219-226.
[37] Judd DL, Winters JD, Stevens-Lapsley JE, et al. Effects of neuromuscular reeducation on hip mechanics and functional performance in patients after total hip arthroplasty: A case series[J]. Clin Biomech (Bristol, Avon), 2016, 32:49-55.
[38] Jassim SS, Douglas SL, Haddad FS. Athletic activity after lower limb arthroplasty: a systematic review of current evidence[J]. Bone Joint J, 2014, 96-B(7):923-927.
[39] Lesch DC, Yerasimides JG, Brosky JA Jr. Rehabilitation following anterior approach total hip arthroplasty in a 49-yearold female: a case report[J]. Physiother Theory Pract, 2010,26(5):334-341.
[40] Stryła W, Pogorzała AM, Rogala P, et al. Algorithm of physical therapy exercises following total hip arthroplasty[J]. Pol Orthop Traumatol, 2013, 78:33-39.
[41] Okoro T, Ramavath A, Howarth J, et al. What does standard rehabilitation practice after total hip replacement in the UK entail? results of a mixed methods study[J]. BMC Musculoskelet Disord, 2013, 14:91.
[42] Peter WF, Nelissen RG, Vlieland TP. Guideline recommendations for post-acute postoperative physiotherapy in total hip and knee arthroplasty: are they used in daily clinical practice[J]? Musculoskeletal Care, 2014, 12(3):125-131.
[43] Heiberg KE, Bruun-Olsen V, Ekeland A, et al. Effect of a walking skill training program in patients who have undergone total hip arthroplasty: Followup one year after surgery[J].Arthritis Care Res (Hoboken), 2012, 64(3):415-423.
[44] Jacobs CA, Lewis M, Bolgla LA, et al. Electromyographic analysis of hip abductor exercises performed by a sample of total hip arthroplasty patients[J]. J Arthroplasty, 2009,24(7):1130-1136.
[45] Yoo JI, Ha YC, Lim JY, et al. Early rehabilitation in elderly after arthroplasty versus internal fixation for unstable intertrochanteric fractures of femur: systematic review and meta-analysis[J]. J Korean Med Sci, 2017, 32(5):858-867.
[46] Di Monaco M, Castiglioni C. Which type of exercise therapy is effective after hip arthroplasty? A systematic review of randomized controlled trials[J]. Eur J Phys Rehabil Med, 2013,49(6):893-907.
[47] Foucher KC, Hurwitz DE, Wimmer MA. Relative importance of gait vs. joint positioning on hip contact forces after total hip replacement[J]. J Orthop Res, 2009, 27(12):1576-1582.
猜你喜欢
临床骨科杂志(2022年3期)2022-11-24
体育科技文献通报(2022年4期)2022-10-21
中华骨与关节外科杂志(2022年1期)2022-08-31
基层中医药(2022年1期)2022-07-22
中国骨与关节杂志(2021年5期)2021-05-29
昆明医科大学学报(2021年1期)2021-02-07
实用临床护理学杂志(电子版)(2020年48期)2020-11-19
浙江临床医学(2020年9期)2020-10-10
World Journal of Clinical Cases(2020年7期)2020-04-23
好日子(2018年9期)2018-10-12
