
A new bleb-independent surgery namely penetrating canaloplasty for corticosteroid-induced glaucoma: a prospective case series
2022-07-30 10:03JingJingHuHaiShuangLinShaoDanZhangWenQingYeJuanGuYanQianXieYiHuaTangYuanBoLiang
INTRODUCTION
Secondary intraocular pressure (IOP) elevation is common in steroid responders to glucocorticoids
. Long-term ocular hypertension may bring with glaucomatous optic nerve damage, that is, corticosteroid-induced glaucoma
. The underlying mechanism may involve increased resistance of aqueous humor in flowing through the trabecular meshwork(TM)
. Besides trabeculectomy
, a standard surgical procedures for glaucoma, corticosteroid-induced high IOP can be managed with trabeculotomy
, trabectome
,nonpenetrating deep sclerectomy
, canaloplasty
,viscocanalostomy
, gonioscopy-assisted transluminal trabeculotomy (GATT)
, Kahook Dual Blade goniotomy
,Ahmed glaucoma valve
, and XEN Gel Stent
. However,their outcomes have not been assessed with large case-control studies.
In this case series, penetrating canaloplasty was successfully performed in all the 10 eyes, and the IOP in 9 eyes was decreased without anti-glaucoma medications. Follow-up data proved the encouraging efficacy and safety of this surgery.
In the development of corticosteroid-induced glaucoma,basement membrane-like materials (positive for type IV collagen) amass in each layer of TM and fine fibrillar materials deposit beneath the inner endothelium of Schlemm’s canal
.We treated corticosteroid-induced glaucoma with penetrating canaloplasty that combines the advantages of canaloplasty(internal filtration and bleb-free) with trabculectomy (a patent communication between the anterior chamber and the Schlemm’s canal but with the sclera flap hermetically sutured).In this surgery, the aqueous humor passes through physiological route
dual conduits: Schlemm’s canal and the passage between the anterior chamber and Schlemm’s canal.Many patients with corticosteroid-induced glaucoma cannot discontinue glucocorticoids due to their primary diseases.Therefore, this dual-channel surgery can prevent the effect of TM’s further lesions during a long term. In the present study,this surgery achieved an ideal control of IOP off medication,suggesting its high efficacy for these patients.
SUBJECTS AND METHODS
3) The illuminated microcatheter (iTrack by iScience Interventional, Menlo Park, CA, USA) was then inserted and advanced through the 360° Schlemm’s canal, until out of the opposite end.
Subjects and Preoperative Examinations All patients were diagnosed with corticosteroid-induced glaucoma that was medically uncontrolled (with a definite history of corticosteroid use, IOP still rises to more than 21 mm Hg under maximal tolerable medical treatment, with concomitant glaucomatous optic disc damage and corresponding visual field defects).
Inclusion criteria: 1) corticosteroid induced high IOP; 2) IOP exceeded 30 mm Hg after maximal medical interventions,despite cessation of corticosteroid therapy (if possible) for at least 3mo; 3) fundus and visual field showed concomitant glaucomatous optic disc damage and corresponding visual field defects; 4) gonioscopy demonstrated wide and open angles and an intact Schlemm’s canal. Exclusion criteria: 1) other secondary glaucoma, 2) refusal to sign the consent form.
Surgery This surgery was pioneered by Dr. Liang YB and patented in the United States (http://patft.uspto.gov/netacgi/nph-Parser?Sect1=PTO2&Sect2=HITOFF&p=1&u=%2F netahtml%2FPTO%2Fsearch-bool.html&r=1&f=G&l=50&co1=AND&d=PTXT&s1=15%2F362,478&OS=15/362,478&RS=15/362,478). All 8 patients (10 eyes) underwent penetrating canaloplasty by an experienced glaucoma surgeon Liang YB. The procedures are listed below.
Use of corticosteroid was recorded. All participants received a comprehensive ophthalmic examination within one week before the surgery, which included best-corrected visual acuity (BCVA), slit-lamp biomicroscopy, gonioscopy,IOP measurement with Goldmann applanation tonometer,fundus examination with a 90 D and non-mydriatic fundus photography, and Humphery SITA standard 24-2 perimetry,and retinal nerve fiber layer assessment with spectral-domain optical coherence tomography (OCT).
“整个世界是一块布,将所有的人串联起来。每个人都与我相联系,我也与他们相联系,就好比披肩的线。拉出其中一根,整个披肩就会塌陷。每个进入我生活的人都影响着披肩的图案。”(389)
另外,三维模型的建立有利于材料统计工作的实施。传统项目中的仪表材料用量通常都是估计量加裕量,主要依靠设计人员的经验来确定,材料用量很难准确控制,容易导致施工中出现纠纷,最终的结果就是材料用量超预算采购量。在三维模型中,设计人员可以根据变送器、接线箱、阀门等仪表设备的位置,准确计算电缆、气源管、支架等各类安装材料数量,大幅提高了材料统计的准确性,既有利于成本控制,也能做到有据可查。
1) A superior rectus traction suture or a corneal bridle traction suture was placed to expose the surgical field, then a fornixbased conjunctival incision and a 4×4 mm
superficial scleral flap of 1/2 scleral thickness were constructed.
2) Beneath the first flap, a smaller and deeper scleral flap(2×2 mm
) was sculpted. A routine paracentesis incision was made to lower the IOP, so as to obviate the risk of trabeculodesceme membrane detachment. Schlemm’s canal was opened and unroofed by the removal of the external wall.The deep scleral flap (2×2 mm
) was then dissected away and both ostia of the canal were repeatedly visco-dilatated with high molecular weight hyaluronic acid (Healon GV), just as procedures in viscocanalostomy.
Ethical Approval This is a prospective interventional study(No.ChiCTR1900020511). The study complied with the tenets of the Declaration of Helsinki and was approved by the Ethics Committee of the eye hospital of Wenzhou Medical University(YX2018-016). Every subject voluntarily signed the consent form.
为了提高土壤肥力,促进核桃生长,在整地的时候也要及时施足基肥,基肥以有机肥为宜,或者选用充分腐熟的农家肥,每亩土地施用有机肥20-30 kg、钙镁磷肥1.5 kg,将肥料与土壤搅拌均匀之后施入定植穴中部,提高土壤肥力。为了提高树苗移植成活率,在移栽之前应该要将幼苗放在水中浸泡3小时左右,或者用泥浆蘸根。苗木栽培的深度可以略微高于幼苗在原来苗圃中的深度,过浅栽培或者过深栽培都不适宜核桃生长。
4) After ligation of a 10-0 polypropylene wire to the distal tip of the microcatheter, the laser microcatheter was retreated.Every two hours, the high polymer sodium hyaluronate (Helon GV, pharmaia company, USA) was injected to expand the Schlemm’s canal with the aid of a special screw-driven syringe.After the withdrawal of the microcatheter, the suture was then replaced in the Schlemm’s canal. After the Schlemm’s canal was fully expanded, the suture was knotted under tension.
5) The trabecular tissue (2×2 mm
) deep at Schlemm’s canal was cut off and forwarded. The respective iris root was cut.
Basic characteristics of the patients are summarized in Table 1.The mean follow-up time was 20.4±13.0mo (range 6-48mo).The mean preoperative IOP and number of anti-glaucoma medications were 45.1±6.5mm Hg and 3.3±0.5, respectively.The mean IOP at 3, 6, 12, 18, 24, 36, and 48mo were 15.8±6.0,14.7±3.3, 15.3±2.0, 15.6±2.6, 17.5±1.8, 16.5±4.9, and 14.0 mm Hg, respectively. The number of anti-glaucoma medications at these time points were all 0 (Table 2). IOP was well controlled in 9 cases off medication, but not reduced in 1 eye of a patient at 1mo after the surgery. Then this patient received ultrasound cycloplasty, trabeculectomy with mitomycin C (MMC), needling subsequently in the following 7mo, but all failed. A drainage valve was implanted at last. At last follow-up, the IOP in this case dropped to 18.5 mm Hg.Gonioscopy confirmed that prolene sutures were precisely positioned within the Schlemm’s canal for the entire follow-up period in all cases. UBM after penetrating canaloplasty shows no subconjunctival filtration bleb (Figure 2). Microhyphaema occurred in 3 eyes, but disappeared within one week through spontaneous absorption. Postoperative transient IOP spike occurred in two eyes which cropped up from one week to one month after surgery. One eye developed choroidal detachment which responded well to conservative treatment. No other complications were observed during or after the surgery. For uveitic eyes, two eyes had no recurrence of the inflammation postoperatively, four eyes had varying degrees of uveitis reactivation and an addition of corticosteroid.
5.面板方差分解技术。面板方差分解分析京津冀城市群土地综合承载力与区域经济发展系统每一个标准差新息冲击对土地综合承载力、人均GDP、地均第二、第三产业增加值变量变化的方差贡献度。[17]首先进行皮尔森(Pearson)相关分析,结果表明,在1%显著性水平下,京津冀城市群土地综合承载力与人均GDP的相关系数为0.984,土地综合承载力与地均第二、第三产业增加值的相关系数为0.972,人均GDP与地均第二、第三产业增加值的相关系数为0.967,系统两两之间存在显著的相关性。因此,根据系统PVAR模型,对LCCC,PGDP和LIIV内生变量进行滞后10期的方差分解(见表5)。
Patients were treated with tobramycin and dexamethasone eye drop and ointment, which were tapered in one month after surgery. IOP and anterior segment were measured after surgery.Follow-up and Outcome Measurements Patients were intensively followed up on the first week after the surgery and the following time points (1, 3, 6, 12, 18, 24, 36, and 48mo). The main observation index included all baseline examinations and IOP, number of glaucoma medications, intraand postoperative complications, and additional interventions.Morphology of the filtering bleb was assessed using slit-lamp microscope and ultrasound biological microscopy (UBM).

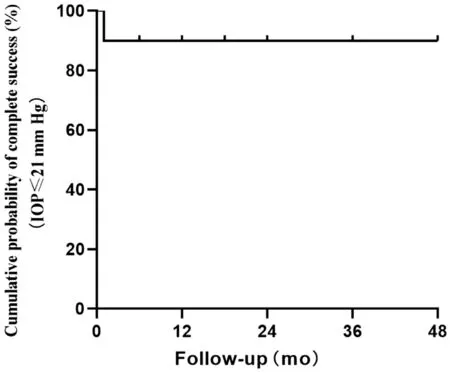
Surgery was defined as success according to postoperative IOP≤21 mm Hg and IOP reduction by ≥20% with (qualified success) or without (complete success) medical treatment.Antiglaucomatous medications were prescribed when IOP was above 21 mm Hg (Figure 1).
Statistical Analysis SPSS Statistics 20.0 (Statistical Product and Service Solutions, IBM, USA) was used for statistical analysis. Student’s
-test was applied to compare IOP values before and after surgery. Value of
<0.05 was considered statistically significant.
经过多次调试和优化,测试结果显示,频率源输出中心频率为24.125 GHz时,其相位噪声可达-87.1 dBc/Hz@1 kHz,如图6所示。
RESULTS
6) Finally, the superficial scleral flap was tightly sutured with 10-0 prolene sutures to ensure a watertight closure preventing any bleb formation. The conjunctival flap was then sutured with 10-0 prolene sutures to the peripheral cornea.


DISCUSSION
Multiple studies have revealed the superiority of canaloplasty to trabeculectomy in treating open angle glaucoma
.Matlach
conducted a prospective randomized clinical trial, showing that canaloplasty and trabeculectomy had comparable IOP-lowering efficacy after 2y for primary open angle glaucoma (POAG), but in the former antimetabolites use and vision-threatening complications were avoided
. Brusini
reported favorable mid-term outcomes of canaloplasty in patients with corticosteroidinduced glaucoma. Researchers have reported successful viscocanalostomy in three cases with corticosteroid-induced glaucoma
.
The average age of 10 cases was 23±13.3y, an age lower than that of POAG cases
. If treated with a routine trabeculectomy,these patients might be plagued with problems related to subconjunctival bleb for a long time. As an internal filtration surgery for restoring the physiological channel, penetrating canaloplasty does not depend on the maintenance of the filtration bleb.
Considering the outflow resistance mainly increases in TM, tension suture aided canaloplasty can be combined with trabeculectomy to bypass the TM, thus channeling the aqueous humor into the expanded Schlemmn’s canal.Since trabeculectomy is a penetrating surgery, we coined this combination as “penetrating canaloplasty”. This surgery can reflect Cairns’s
concept, in which aqueous humor is drained through trabeculectomy-formed fistula into the Schlemm’s canal, thus realizing the internal filtration. Our previous study has reported a favorable outcome of penetrating canaloplasty in primary angle-closure glaucoma
and traumatic angle recession glaucoma
. Herein we presented the preliminary surgical outcomes of penetrating canaloplasty for corticosteroid-induced glaucoma.
观察组患者采取ACEI药物治疗,10 mg/d的苯那普利,对于高血压患者降压效果不好可加至20 mg/d,对照组患者采取非ACEI药物治疗,使用钙离子拮抗剂、β受体阻断剂等。两组患者治疗时间均为3个月。
In the present study, the mean IOP values at postoperative seven time points were favorable for these young patients.Literature shows viscocanalostomy and canaloplasty have the potential to reduce IOP among mid-teens and lower-teens,respectively
. Penetrating canaloplasty is expected to be a promising treatment option for reducing IOP to lower- and mid-teens with corticosteroid-induced glaucoma.
Microhyphaema was the most common surgery-related complication, perhaps due to the blood reflux from the episcleral veins or the collateral damage to iris. Two cases developed postoperative IOP spike between one week and one month after surgery. It may be related to the structural collapse of internal drainage channel caused by long-term high IOP. We hypothesize that there is a time window for the resuscitation of internal drainage channel, so close observation and appropriate intervention should be conducted for these patients. One eye developed choroidal detachment but responded well to conservative treatment. Other reported canaloplasty-related adverse events in POAG include Descemet’s membrane detachment, cataract formation, suture extrusion
. But these events were not observed in this study.
This study lacks of control group. Prospective and randomized studies with better designs and sufficient samples were needed to verify the effectiveness of the surgery.
“现在已经处于价格的底点,未来价格将稍有反弹并逐渐趋于平稳。”杨同宇认为,磷复肥会议结束后,许多肥料厂家已陆续出台了订肥政策。进入12月份,将进入生产、备肥的关键时期,需求将逐渐显现,并为市场提供支撑。
In conclusion, penetrating canaloplasty is effective for corticosteroid-induced glaucoma without any serious complications, making it a viable or preferred surgical choice.
ACKNOWLEDGEMENTS
Supported by National Key Research and Development Project of China (No.2020YFC2008200);Program for Zhejiang Leading Talent of S&T Innovation(No.2021R52012); Key Research and Development Projects of Zhejiang Province (No.2022C03112); Zhejiang Provincial Program for the Cultivation of Leading Talents in Colleges and Universities (No.2020099).
Conflicts of Interest: Hu JJ, None; Lin HS, None; Zhang SD, None; Ye WQ, None; Gu J, None; Xie YQ, None; Tang YH, None; Liang YB, None.
1 Becker B. Intraocular pressure response to topical corticosteroids.
1965;4:198-205.
2 Chan WL, Wiggs JL, Sobrin L. The genetic influence on corticosteroidinduced ocular hypertension: a field positioned for discovery.
2019;202:1-5.
3 Jones R 3rd, Rhee DJ. Corticosteroid-induced ocular hypertension and glaucoma: a brief review and update of the literature.
2006;17(2):163-167.
4 Razeghinejad MR, Katz LJ. Steroid-induced iatrogenic glaucoma.
2012;47(2):66-80.
5 Roberti G, Oddone F, Agnifili L, Katsanos A, Michelessi M,Mastropasqua L, Quaranta L, Riva I, Tanga L, Manni G. Steroidinduced glaucoma: Epidemiology, pathophysiology, and clinical management.
2020;65(4):458-472.
6 Clark AF, Wordinger RJ. The role of steroids in outflow resistance.
2009;88(4):752-759.
7 Sihota R, Konkal VL, Dada T, Agarwal HC, Singh R. Prospective,long-term evaluation of steroid-induced glaucoma.
(
)2008;22(1):26-30.
8 Jonas JB, Degenring RF, Kamppeter BA. Outcome of eyes undergoing trabeculectomy after intravitreal injections of triamcinolone acetonide.
2004;13(3):261.
9 Honjo M, Tanihara H, Inatani M, Honda Y. External trabeculotomy for the treatment of steroid-induced glaucoma.
2000;9(6):483-485.
10 Dang YL, Kaplowitz K, Parikh HA, Roy P, Loewen RT, Francis BA, Loewen NA. Steroid-induced glaucoma treated with trabecular ablation in a matched comparison with primary open-angle glaucoma.
2016;44(9):783-788.
11 Elhofi A, Helaly HA. Outcome of primary nonpenetrating deep sclerectomy in patients with steroid-induced glaucoma.
2018;2018:9215650.
12 Brusini P, Tosoni C, Zeppieri M. Canaloplasty in corticosteroidinduced glaucoma. preliminary results.
2018;7(2):E31.
13 Krishnan R, Kumar N, Wishart PK. Viscocanalostomy for refractory glaucoma secondary to intravitreal triamcinolone acetonide injection.
2007;125(9):1284-1286.
14 Boese EA, Shah M. Gonioscopy-assisted transluminal trabeculotomy(GATT) is an effective procedure for steroid-induced glaucoma.
2019;28(9):803-807.
15 Epstein R, Taravella M, Pantcheva MB. Kahook Dual Blade goniotomy in post penetrating keratoplasty steroid-induced ocular hypertension.
2020;19:100826.
16 Eksioglu U, Oktem C, Sungur G, Yakin M, Demirok G, Ornek F.Outcomes of Ahmed glaucoma valve implantation for steroid-induced elevated intraocular pressure in patients with retinitis pigmentosa.
2018;38(5):1833-1838.
17 Rezkallah A, Mathis T, Denis P, Kodjikian L. XEN gel Stent to treat intraocular hypertension after dexamethasone-implant intravitreal injections: 5 cases.
2019;28(1):e5-e9.
18 Riva I, Brusini P, Oddone F, Michelessi M, Weinreb RN, Quaranta L.Canaloplasty in the treatment of open-angle glaucoma: a review of patient selection and outcomes.
2019;36(1):31-43.
19 Zhang B, Kang J, Chen XM. A system review and Meta-analysis of canaloplasty outcomes in glaucoma treatment in comparison with trabeculectomy.
2017;2017:2723761.
20 Matlach J, Dhillon C, Hain J, Schlunck G, Grehn F, Klink T.Trabeculectomy versus canaloplasty (TVC study) in the treatment of patients with open-angle glaucoma: a prospective randomized clinical trial.
2015;93(8):753-761.
21 Rulli E, Biagioli E, Riva I, Gambirasio G, de Simone I, Floriani I,Quaranta L. Efficacy and safety of trabeculectomy vs nonpenetrating surgical procedures: a systematic review and meta-analysis.
2013;131(12):1573-1582.
22 Kim EA, Law SK, Coleman AL, Nouri-Mahdavi K, Giaconi JA,Yu F, Lee JW, Caprioli J. Long-term bleb-related infections after trabeculectomy: incidence, risk factors, and influence of bleb revision.
2015;159(6):1082-1091.
23 Cairns JE. Trabeculectomy. Preliminary report of a new method.
1968;66(4):673-679.
24 Cheng HH, Hu C, Meng JY, Zhang SD, Lin SG, Bao JY, Xie YQ, Le RR, Ye C, Liang YB. Preliminary efficacy of penetrating canaloplasty in primary angle-closure glaucoma.
2019;55(6):448-453.
25 Zhang SD, Hu C, Cheng HH, Gu J, Samuel K, Lin HS, Deng YX,Xie YQ, Hu JJ, Le RR, Xu SX, Tham CC, Liang YB. Efficacy of bleb-independent penetrating canaloplasty in primary angle-closure glaucoma: one-year results.
2022;100(1):e213-e220.
26 Cheng HH, Ye WQ, Zhang SD, Xie YQ, Gu J, Le RR, Deng YX, Hu C, Zhao ZQ, Ke ZS, Liang YB. Clinical outcomes of penetrating canaloplasty in patients with traumatic angle recession glaucoma: a prospective interventional case series.
2022:bjophthalmol-bjophtha2021-320659.
27 Tektas OY, Lütjen-Drecoll E. Structural changes of the trabecular meshwork in different kinds of glaucoma.
2009;88(4):769-775.
28 Grieshaber MC. Viscocanalostomy and canaloplasty:
schlemm’s canal surgery.
2017;59:113-126.
29 Cagini C, Peruzzi C, Fiore T, Spadea L, Lippera M, Lippera S.Canaloplasty: current value in the management of glaucoma.
2016;2016:7080475.
30 Konopińska J, Mariak Z, Rękas M. Improvement of the safety profile of canaloplasty and phacocanaloplasty: a review of complications and their management.
2020;2020:8352827.
猜你喜欢
安徽农学通报(2022年6期)2022-04-07
西部交通科技(2021年9期)2021-01-11
山西农经(2020年13期)2020-07-14
投资北京(2018年1期)2018-01-22
意林·少年版(2018年23期)2018-01-05
初中生世界·九年级(2017年10期)2017-11-08
投资北京(2017年1期)2017-02-13
投资北京(2016年10期)2016-11-23
股市动态分析(2016年15期)2016-10-19
中学生数理化·八年级数学人教版(2016年5期)2016-08-23
 International Journal of Ophthalmology2022年7期
International Journal of Ophthalmology2022年7期
- International Journal of Ophthalmology的其它文章
- Impact of OCT scan-patterns in identifying morphological features of lamellar macular holes and macular pseudoholes
- Virtual reality training improves accommodative facility and accommodative range
- Short-term effect of 0.01% atropine sulphate eye gel on myopia progression in children
- Reduced choroidal peripapillary capillaries in thyroidassociated ophthalmopathy with early stage of dysthyroid optic neuropathy
- Incidence of ocular manifestations in patients with graft versus host disease after allogeneic stem cell transplant in Riyadh, Saudi Arabia
- Clinical features, surgical outcomes and genetic analysis of ectodermal dysplasia with ocular diseases