
Incidence and risk factors for vitreous loss in residents performing manual small-incision cataract surgery
2022-07-30 10:03RajeshSubhashJoshiAshokHukumchandMadanPreetiDashrathWadekarNiveditaPatilSonaliTamboliTanmaySurwadeNamrataBansode
INTRODUCTION
Selection of material and writing the text: Archakova T Design and correction of the review: Nedosugova L
Gupta
noted that intraoperative complications are more in left-eye operated MSICS patients than in those with right eye surgery; the reason stated was that the nasal bridge of the patients hinders free movement of right-handed surgeons. This finding is in contrast with the findings of our study, where vitreous loss was observed equally in the right and left eye(
=5,
=0.15), and none of the surgeons in our study were lefthanded.
SUBJECTS AND METHODS
法律上的人格,本质上指人的资格,即成为法律关系主体的资格,[注]黄军锋、千省利:《论胎儿的法律人格及利益保护》,《西安交通大学学报(社会科学版)》2011年第3期,第64—69页。故法律人格亦可被理解为法律认可的一种享受权利、承担义务的资格。事实上,在当前人工智能高速发展并已开始投入应用的环境下,此一问题已远非是“科幻”式的,法律实践和研究都必须直面之。在不少关于人工智能和法律的讨论中,学者开始留意到了人工智能的法律人格问题,专门的探讨也已出现。[注]袁曾:《人工智能有限法律人格审视》,《东方法学》2017年第5期,第50—57页。
The present retrospective record review study was performed in 490 patients undergoing cataract surgeries through the MSICS technique from November 2018 to December 2019 by 7 third-year residents (JR3) at a tertiary eye care center,which is providing free cataract services in central India.Patients assigned to the residents during the course of their residency were considered and was not a continuous allotment.The study population included patients visiting to the hospital for consultation and admitted to the hospital for cataract surgery. Data on age; sex; history of trauma, diabetes mellitus,hypertension, and cardiac problems; corrected distance visual acuity; intraocular pressure; anterior chamber (AC)depth (derived from optical biometry); slit-lamp examination after pupillary dilatation for evidence of pseudoexfoliation and subluxation of cataract; and grade of cataract were collected. Retinal examination was performed using indirect ophthalmoscopy.
To the best of our knowledge, none of the studies on MSICS have focused on the most vital complication of cataract surgery, namely vitreous loss. The present study was conducted in residents having performed an average of 68 MSICS; therefore, more complications were expected.However, each case was supervised by a senior surgeon, who intervened in case of any complication. Supervised MSICS learning has shown vitreous loss in one case out of 52 patients stressing the significance of supervision
. Hashemi
reported a vitreous loss rate of 10.2% in unsupervised cataract surgery by residents. Supervision assists not only in avoiding intraoperative complications but also in case selection
.Patients with a shallow AC, subluxation, uncooperative attitude,small pupil, traumatic cataract, post-vitrectomized eyes, glaucoma,and pseudoexfoliation were excluded from the study.
Cataract surgery is the most commonly performed eye surgery in the world
. Despite significant development in the technique of cataract surgery, the burden of blindness due to cataract continues to increase in developing countries
.Thus, competent ophthalmologists capable of performing cataract surgery without any complications are highly required.Most of the cataracts in the Asian population are hard cataracts because patients generally present late for surgery
. Manual small-incision cataract surgery (MSICS) is the preferred technique for cataract removal in developing countries
.The MSICS technique involves the creation of a self-sealing sclerocorneal tunnel, removal of nucleus through the tunnel,and placement of an intraocular lens (IOL) inside the capsular bag. The technique is popular in developing countries because of less investment required and its low cost, less dependency on machine, rapidity, and excellent outcomes with a low complication rate
. MSICS can be performed in hard,brown, and black cataractous lenses. Phacoemulsification cataract surgery in such cataracts may cause high ultrasonic power consumption with effect on the corneal endothelium.Manipulation of such hard cataracts may lead to zonular weakness. The residency program in developing countries focuses on providing training in extracapsular cataract extraction and MSICS, whereas the residency program in developed countries focuses on phacoemulsification as the preferred method for cataract surgery
.
Immature senile cataract, irrigation and aspiration of cortical material, and anterior capsular extension are independent risk factors for vitreous loss. Our findings may serve as a guide for future trainers or residents learning MSICS.
Statistical Analysis Data were entered in an MS Excel sheet,and statistical analysis was performed using SPSS version 13.0 (SPSS Inc, Chicago, IL, USA). The data are expressed as mean±standard deviation (SD) or number and percentage.Fisher’s exact test was used for categorical variables, whereas the Student’s
-test was used for continuous variables. The confidence interval (CI) for calculation of the odds ratio (OR)was 95%. Univariate and multivariate Logistic regressions were performed for the factors responsible for vitreous loss,and a
value of <0.05 was considered statistically significant.
RESULTS
The mean age of the participants at the time of surgery was 68.42±2.05y, with a range of 62-78y. Of the 490 patients, 250 patients were male and 240 patients were female (
=0.23).Of the total surgeries performed, 205 (41.8%) surgeries were performed on the right eye and 285 (58.1%) surgeries were performed on the left eye. Among the cases allotted to the residents, 215 (43.9%) cases exhibited mature white cataract,185 (37.8%) cases exhibited brown cataract, and 90 (18.3%)cases exhibited immature senile cataract. Each resident included in the study had performed an average of 68 surgeries(range 45-80).
在传统课堂教学中,节奏慢,课堂容量小,教学方式比较单调呆板。多媒体教学可将抽象复杂的理论形象地表现出来,减少教师的重复工作,使教师的活动不像以前:一张嘴、一支粉笔、一块黑板加简单电教手段组成。利用多媒体教学呈现信息量大,速度快,图文并茂的优势,能使学生更好更快地接受知识,提高教学效率。
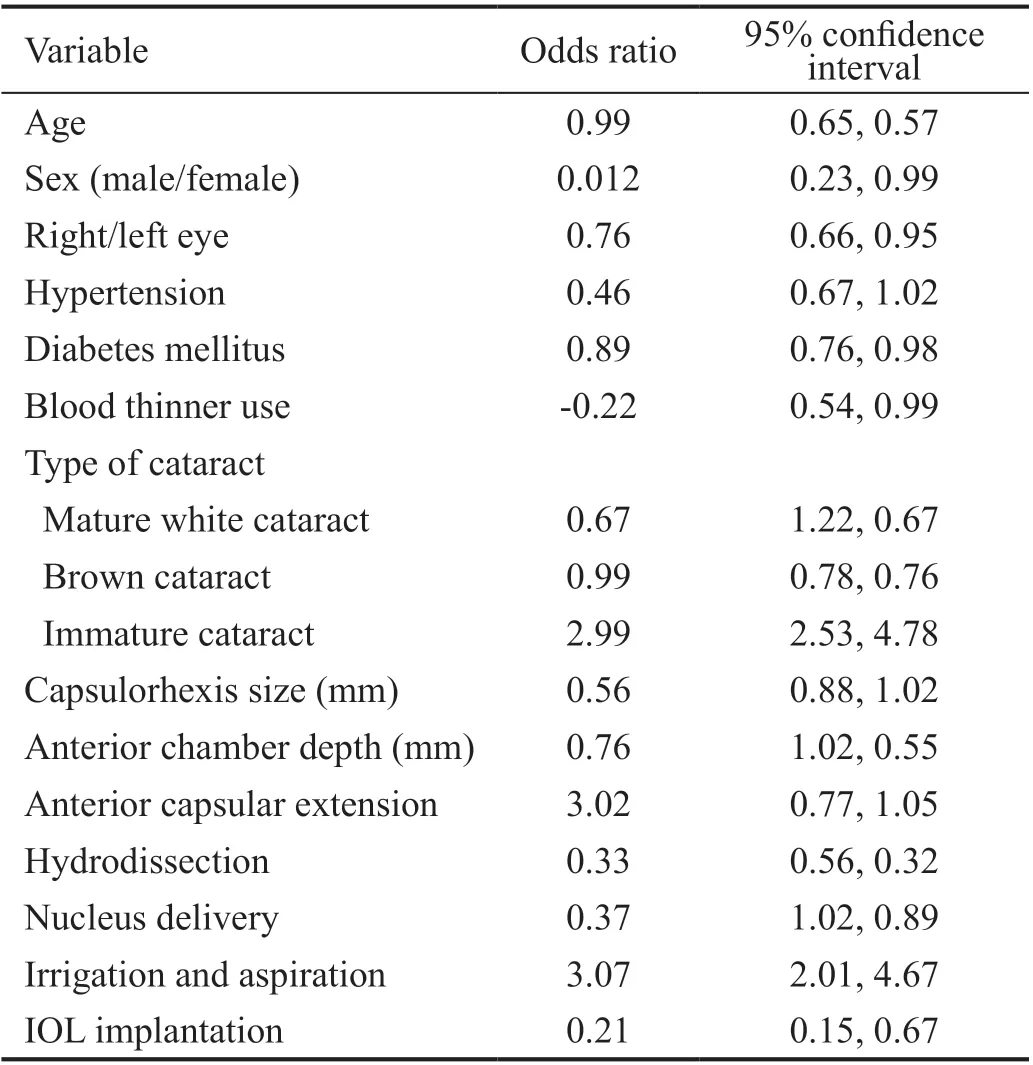
The incidence of intraoperative vitreous loss was 2% (10/490),and 5 eyes (1%) developed PCR without vitreous loss. Vitreous loss occurred during hydrodissection [1/10 (10%)], nucleus delivery [3/10 (30%)], irrigation and aspiration [5/10 (50%)],and IOL insertion [1/10 (10%)]. Patient who had vitreous loss during hydrodissection and nucleus drop required nucleus removal, pars plana vitrectomy, and scleral fixation of IOL. In patients having vitreous loss during irrigation and aspiration of the cortical matter, anterior vitrectomy was performed and placement of IOL over the rim of anterior capsule was done.None of the patient remained aphakic. Patients having zonular dehiscence were fixed with endocapsular ring and an anterior vitrectomy was done and IOL was placed in the capsular bag.Table 1 illustrates the association between the clinical characteristics and vitreous loss. Systemic factors, such as diabetes mellitus and hypertension, and ocular factors, such as AC depth and size of the capsulorhexis, did not exhibit any correlation with the vitreous loss. On univariate Logistic regression analysis (Table 2), a statistically significant association of vitreous loss with immature cataract (OR=2.99;
=0.04), irrigation and aspiration (OR=3.07;
=0.02), and anterior capsular extension (OR=3.02;
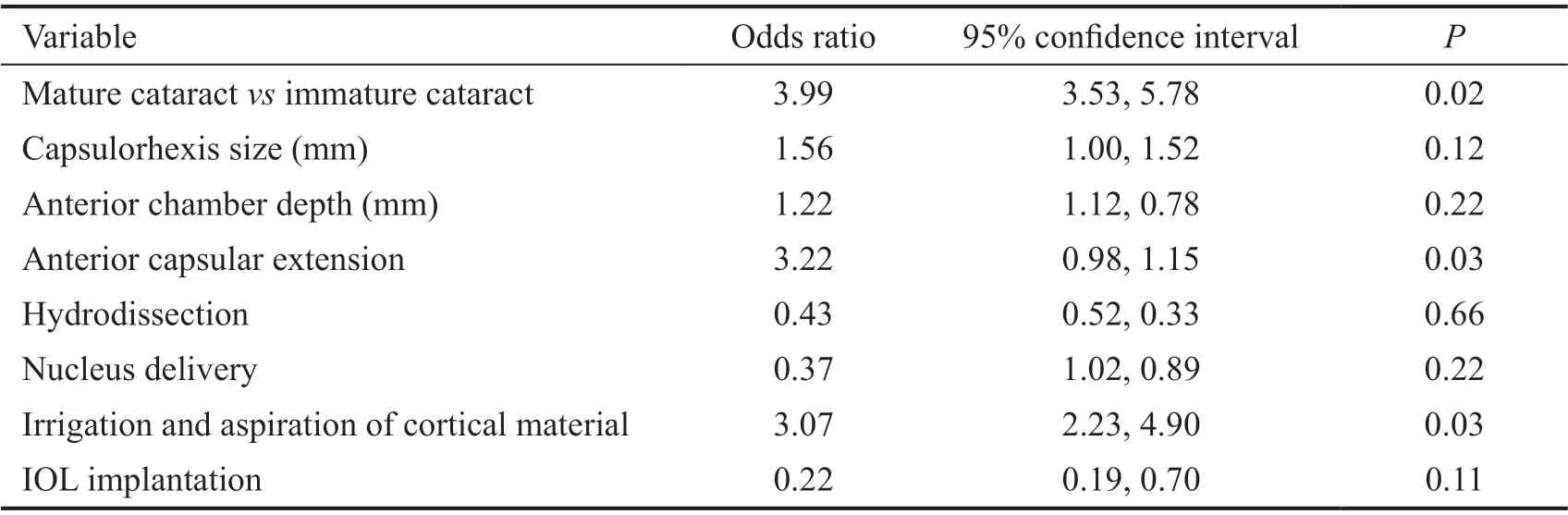
=0.04) was observed.Multivariate stepwise Logistic regression analysis (Table 3)also confirmed immature senile cataract (OR=3.99;
=0.02),irrigation and aspiration of cortical material (OR=3.07;
=0.03), and anterior capsular extension (OR=3.22,
=0.03)as independent risk factors for vitreous loss.
DISCUSSION
Vitreous loss is the major intraoperative complication of cataract surgery. The present study indicated a vitreous loss rate of 2% in MSICS. This rate is higher than that reported in a study by Haripriya
, who reported a vitreous loss rate of 0.64% in MSICS when they compared the complication rates between phacoemulsification and MSICS; this difference may be because staff and trainee surgeons were included as participants in the study, whereas the present study included only JR3 students. Lynds
reported the incidence rate of vitreous loss of 1.9% in a supervised residents training at alarge urban United States residency training program. Gupta
exhibited a posterior capsular rupture with a vitreous loss rate of 1.76% in their study on the learning curve for MSICS in a tertiary eye care center in residents entering second postgraduate residency.In the present study five eyes (1%) exhibited PCR; however,no vitreous loss was observed. The IOL was safely placed in the capsular bag. The vitreous loss after PCR can be avoided by plugging the rent with high molecular weight OVD. This helps to maintain the AC and prevent the extension of PCR.The rate of PCR in MSICS reported in various studies varies from 0.14% to 1.9%
. This finding is in contrast to those of studies, which have reported the rate of vitreous loss ranging from 3.8% to 5.1% and on the higher side in surgeries performed by residents learning phacoemulsification
. This could be due to steeper learning curve for phacoemulsification.Subudhi
have shown steep learning curve for residents performing MSICS.

Reasons for inconsistencies in the reported vitreous loss rates in various studies on MSICS could be due to differences in the surgical technique, exclusion criteria, training program schedules in the institutes, and supervised or unsupervised training. Designing of a surgical schedule may ensure uniformity in postgraduate training in surgical procedures
.PCR identification is crucial to prevent further postoperative complications occurring due to vitreous loss. The number of cataract surgeries performed by the residents influences the rate of intraoperative complications. Gupta
observed that surgeries performed by residents having performed an average of 100 surgeries are thrice more likely to exhibit intraoperative complications than those performed by residents who have already performed 600 surgeries.
Ethical Approval The study was approved by the Institutional Ethics Committee and was performed in accordance with the Declaration of Helsinki. Written informed consent was obtained from the subject and none of the participants received any finances.
Patients with only one functional eye, pseudoexfoliation,subluxated cataract, post-vitrectomized eye, posterior polar cataract, primary open or closed angle glaucoma, traumatic cataract, and all types of complicated cataract were excluded from the study.
Gupta
observed that older patients exhibit higher intraoperative complications than younger patients. Similar observation were made by Hashemi
and Blomquist
. However, no such preponderance was reported in our study.
Vitreous loss is a serious complication of cataract surgery that is responsible for the suboptimal visual outcome after cataract surgery
. It may lead to retinal detachment,glaucoma, cystoid macular edema, persistent corneal edema,and IOL displacement. A study conducted in Aravind Eye Hospital, Madurai, compared the intraoperative complication rate between phacoemulsification, MSICS, and largeincision extracapsular cataract extraction performed by trainee surgeons and reported that the complication rate with phacoemulsification is significantly higher than with MSICS
.Gupta
reported a vitreous loss rate of 1.85% in MSICS performed by residents who were learning MSICS.Haripriya
reported vitreous loss rates of 0.87% and 0.64% in phacoemulsification and MSICS, respectively. Lynds
also reported a vitreous loss rate of 1.9% in a small series of MSICS. Haripriya
studied the intraoperative complication rates of phacoemulsification, MSICS, and large-incision extracapsular cataract extraction performed by staff surgeons well trained in all types of cataract surgeries,fellowship students in their postresidency training, visiting trainees who were practicing ophthalmologists, and residents enrolled for the postgraduation program. However, to the best of our knowledge, none of the studies have focused on determining the incidence of vitreous prolapse and correlative factors associated with vitreous loss in the central Indian population in a tertiary eye care center.
The present study identified preoperative factors, such as immature senile cataract (OR=3.99;
=0.02), and intraoperative factors, such as irrigation and aspiration of cortical material(OR=3.07;
=0.03) and anterior capsular extension (OR=3.22,
=0.03), as independent risk factors for vitreous loss on multivariate analysis. Studies on phacoemulsification have reported that mature and hard nuclear cataract are associated with vitreous loss in surgeries performed by residents
.Additionally, Gupta
exhibited that intraoperative complications are more in eyes having mature and hard cataract; however, due to lack of preoperative data on the cataract morphology, they used preoperative visual acuity as an indicator for the hardness and maturity of cataract. In the present study, 6 eyes with immature cataract and 2 eyes each with mature white, and brown cataract exhibited vitreous loss.Prolapsing the nucleus out of the capsular bag is difficult in immature cataract with small capsulorhexis. Damage to the zonular fibers may occur with repeated attempts to prolapse nucleus into the AC. Cases having zonular dehiscence,capsular bag was fixed with a capsular tension ring and an anterior vitrectomy was performed. Haripriya
also noted the vitreous loss rate of 1.85% with zonular dehiscence in MSICS. Gupta
noted a vitreous loss rate of 0.37% with zonular dehiscence. Furthermore, removal of cortical matter from the equatorial area becomes challenging if pupil becomes small. Moreover, a tendency of blind aspiration of cortical fibers is present in a small pupil. Conversely, no or little cortex is required to be cleared from the AC in a mature cataract.Cortical removal must be performed carefully.
Extended anterior capsulorhexis is another crucial factor influencing vitreous loss (OR=3.22,
=0.03). Hashemi
also identified anterior capsular tear as an independent factor for vitreous loss in surgeries performed by residents learning phacoemulsification. In MSICS, shallow AC may occur during nucleus expression. Therefore, the likelihood of extension of the anterior capsular tear toward the posterior capsule is high.AC formation with OVD does help to prevent extension of anterior capsular tear to the posterior capsule.
Hydrodissection (
=1) and IOL implantation (
=1) are another vital step associated with vitreous loss. Patient who exhibited vitreous loss after hydrodissection had mature cataract. This patient required pars plana vitrectomy, nucleus removal, and scleral fixated IOL.
At our institute, training for MSICS starts at the end of first year of JR1. Procedures that are taught initially include the construction of a scleral tunnel, creation of a side port, staining of the anterior capsule with trypan blue dye, CCC, and hydrodissection in a stepwise and supervised manner. The stepwise learning helps in reducing complications. Additionally, students are trained in performing phacoemulsification. Simulator based learning has been shown to reduce complications while performing cataract surgery
.The present study has certain limitations. The study was performed at a single center in a retrospective manner with limited number of participants who were in their third year of residency. Although the data were collected from electronic medical records, multiple surgeons were involved in the supervision of the residents. Being a nonrandomized study,the study is prone to case selection bias; however, guidelines regarding the type of cataract to be allotted to the residents in training was difficult to formulate. Residents require strict supervision while performing certain steps of MSICS such as capsulorhexis, nucleus delivery, and cortical aspiration.
Thus, a vitreous loss rate of 2% was observed in our study. On multivariate analysis, preoperative factor, namely immature senile cataract, and intraoperative factors, namely irrigation and aspiration of cortical material and anterior capsular extension, were identified as independent risk factors for vitreous loss. These findings may serve as a guide for future trainers or residents learning MSICS.
针对现有关联度的缺陷,本文提出完全加权正项集PI(Positive Itemset)关联度(all-weighted PI Relevancy,awPIR)的计算如式(8)所示:
ACKNOWLEDGEMENTS
Conflicts of Interest: Joshi RS, None; Madan AH, None;Wadekar PD, None; Patil N, None; Tamboli S, None;Surwade T, None; Bansode N, None.
1 Yoshizaki M, Ramke J, Zhang JH, Aghaji A, Furtado JM, Burn H,Gichuhi S, Dean WH, Congdon N, Burton MJ, Buchan J. How can we improve the quality of cataract services for all? A global scoping review.
2021;49(7):672-685.
2 Lou LX, Wang JY, Xu PF, Ye X, Ye J. Socioeconomic disparity in global burden of cataract: an analysis for 2013 with time trends since 1990.
2017;180:91-96.
3 Flaxman SR, Bourne RRA, Resnikoff S, Ackland P, Braithwaite T,Cicinelli MV, Das A, Jonas JB, Keeffe J, Kempen JH, Leasher J,Limburg H, Naidoo K, Pesudovs K, Silvester A, Stevens GA, Tahhan N, Wong TY, Zheng YF. Global causes of blindness and distance vision impairment 1990-2020: a systematic review and meta-analysis.
2017;5(12):e1221-e1234.
4 Joshi RS, Singanwad SV. Frequency and surgical difficulties associated with pseudoexfoliation syndrome among Indian rural population scheduled for cataract surgery: hospital-based data.
2019;67(2):221-226.
5 Fang Z, Chen XY, Lou LX, Yao K. Socio-economic disparity in visual impairment from cataract.
2021;14(9):1310-1314.
6 Joshi RS, Muley SJ. Combined 30-degree bevel up and down technique against 0-degree phaco tip for phacoemulsification surgery of hard cataracts.
2017;11:1073-1079.
7 Haripriya A, Chang DF, Reena M, Shekhar M. Complication rates of phacoemulsification and manual small-incision cataract surgery at Aravind Eye Hospital.
2012;38(8):1360-1369.
8 Sen A. Six years after manual small incision cataract surgery-Perspective from a secondary level eye hospital in Rural India.
2021;69(3):590-593.
9 Venkatesh R, Tan CSH, Sengupta S, Ravindran RD, Krishnan KT,Chang DF. Phacoemulsification versus manual small-incision cataract surgery for white cataract.
2010;36(11):1849-1854.
10 Bernhisel A, Pettey J. Manual small incision cataract surgery.
2020;31(1):74-79.
11 Ruit S, Gurung R, Vyas S. The role of small incision suture-less cataract surgery in the developed world.
2018;29(1):105-109.
12 Kaplowitz K, Yazdanie M, Abazari A. A review of teaching methods and outcomes of resident phacoemulsification.
2018;63(2):257-267.
13 Borboli-Gerogiannis S, Jeng-Miller KW, Koulisis N, Moustafa GA,Chang KK, Chen SH, Gardiner MF, Greenstein SH, Luo ZH, Chen TC,Loewenstein JI, Miller JW, Haviland MJ, Kloek CE. A comprehensive surgical curriculum reduced intra-operative complication rates of resident-performed cataract surgeries.
2019;76(1):150-157.
14 Johansson B, Lundström M, Montan P, Stenevi U, Behndig A. Capsule complication during cataract surgery: long-term outcomes: Swedish Capsule Rupture Study Group report 3.
2009;35(10):1694-1698.
15 Thevi T, Abas AL. Vitreous loss-causes, associations, and outcomes:eight-year analysis in Melaka Hospital.
2018;11(2):113-118.
16 Aaronson A, Viljanen A, Kanclerz P, Grzybowski A, Tuuminen R.Cataract complications study: an analysis of adverse effects among 14, 520 eyes in relation to surgical experience.
2020;8(22):1541.
17 Gupta S, Haripriya A, Vardhan SA, Ravilla T, Ravindran RD.Residents' learning curve for manual small-incision cataract surgery at aravind eye hospital, India.
2018;125(11):1692-1699.
18 Lynds R, Hansen B, Blomquist PH, Mootha VV. Supervised resident manual small-incision cataract surgery outcomes at large urban United States residency training program.
2018;44(1):34-38.
19 Hashemi H, Mohammadpour M, Jabbarvand M, Nezamdoost Z,Ghadimi H. Incidence of and risk factors for vitreous loss in residentperformed phacoemulsification surgery.
2013;39(9):1377-1382.
20 Quillen DA, Phipps SJ. Visual outcomes and incidence of vitreous loss for residents performing phacoemulsification without prior planned extracapsular cataract extraction experience.
2003;135(5):732-733.
21 Woodfield AS, Gower EW, Cassard SD, Ramanthan S. Intraoperative phacoemulsification complication rates of second- and third-year ophthalmology residents a 5-year comparison.
2011;118(5):954-958.
22 Bai HQ, Yao L, Wang HT. Clinical investigation into posterior capsule rupture in phacoemulsification operations performed by surgery trainees.
2020;2020:1317249.
23 Subudhi P, Patro S, Subudhi BNR, Sitaram S, Khan Z, Mekap C.Resident performed sutureless manual small incision cataract surgery(MSICS):outcomes.
2021;15:1667-1676.
24 Gogate P. Effect of wet-laboratory training on resident-performed manual small-incision cataract surgery.
2018;66(6):798.
25 Roohipoor R, Yaseri M, Teymourpour A, Kloek C, Miller JB,Loewenstein JI. Early performance on an eye surgery simulator predicts subsequent resident surgical performance.
2017;74(6):1105-1115.
26 Gharaee H, Jahani M, Banan S. A comparative assessment of intraoperative complication rates in resident-performed phacoemulsification surgeries according to najjar-awwad preoperative risk stratification.
2020;14:1329-1336.
27 Blomquist PH, Morales ME, Tong LY, Ahn C. Risk factors for vitreous complications in resident-performed phacoemulsification surgery.
2012;38(2):208-214.
28 Zare M, Javadi MA, Einollahi B, Baradaran-Rafii AR, Feizi S, Kiavash V. Risk factors for posterior capsule rupture and vitreous loss during phacoemulsification.
2009;4(4):208-212.
29 Nair AG, Ahiwalay C, Bacchav AE, Sheth T, Lansingh VC, Vedula SS,Bhatt V, Reddy JC, Vadavalli PK, Praveen S, Wairagade NA, Pettey J.Effectiveness of simulation-based training for manual small incision cataract surgery among novice surgeons: a randomized controlled trial.
2021;11(1):10945.
30 Dean WH, Gichuhi S, Buchan JC, Makupa W, Mukome A, Otiti-Sengeri J, Arunga S, Mukherjee S, Kim MJ, Harrison-Williams L,MacLeod D, Cook C, Burton MJ. Intense simulation-based surgical education for manual small-incision cataract surgery: the ophthalmic learning and improvement initiative in cataract surgery randomized clinical trial in Kenya, Tanzania, Uganda, and Zimbabwe.
2021;139(1):9-15.
猜你喜欢
故事作文·高年级(2019年11期)2019-12-01
智富时代(2019年2期)2019-04-18
智富时代(2019年2期)2019-04-18
党的生活·党员电教与远程教育(2017年9期)2017-10-17
少年文艺·开心阅读作文(2017年4期)2017-04-07
东方教育(2016年6期)2017-01-16
儿童故事画报(2015年12期)2016-01-25
党的生活·党员电教与远程教育(2015年4期)2015-04-07
小樱桃·童年阅读(2014年10期)2014-11-03
知识窗(2009年10期)2009-12-01
 International Journal of Ophthalmology2022年7期
International Journal of Ophthalmology2022年7期
- International Journal of Ophthalmology的其它文章
- Impact of OCT scan-patterns in identifying morphological features of lamellar macular holes and macular pseudoholes
- Virtual reality training improves accommodative facility and accommodative range
- Short-term effect of 0.01% atropine sulphate eye gel on myopia progression in children
- Reduced choroidal peripapillary capillaries in thyroidassociated ophthalmopathy with early stage of dysthyroid optic neuropathy
- Incidence of ocular manifestations in patients with graft versus host disease after allogeneic stem cell transplant in Riyadh, Saudi Arabia
- Clinical features, surgical outcomes and genetic analysis of ectodermal dysplasia with ocular diseases