
经桡动脉和经股动脉路径同期进行冠状动脉三支病变介入治疗患者住院期间及长期临床结果比较
2015-12-15 09:01李佳徐晗窦克非徐波尤士杰吴永健乔树宾颜红兵杨跃进
中国循环杂志 2015年4期
李佳,徐晗,窦克非,徐波,尤士杰,吴永健,乔树宾,颜红兵,杨跃进
冠心病研究
经桡动脉和经股动脉路径同期进行冠状动脉三支病变介入治疗患者住院期间及长期临床结果比较
李佳,徐晗*,窦克非,徐波,尤士杰,吴永健,乔树宾,颜红兵,杨跃进
目的:通过与经股动脉(TF)径路比较,评价经桡动脉(TR) 径路同期进行经皮冠状动脉(冠脉)介入治疗冠脉三支病变的安全性、可行性、住院期间及长期随访期间临床结果。
方法:4 974例冠脉造影诊断为左主干未受累的冠脉三支病变并接受单次经皮血运重建治疗的患者入选了本项研究。分为TR组3 856例,TF组1 118例。手术和临床结果通过数据库和随访获得。本研究应用倾向评分匹配方法得到基线资料均衡的930对患者来比较TR组和TF组的住院期间和长期随访期间临床结果,用Cox比例风险模型评估两组间所有临床结果的风险差异,用Kaplan-Meier法估算两组安全性和有效性相关事件的累积发生率,并用logrank法进行比较。
结果:倾向评分匹配后,两组的临床和血管造影特征无统计学意义。TR组较TF组住院时间更短[(7.49±4.46)天vs(8.63±6.23)天,P<0.0001]、出血事件更少(1.1%vs 2.9%,P=0.003)外,其余手术结果差异无统计学意义。临床随访显示TR组全因死亡率明显降低(TR组1.8%,TF组4.2%,P=0.0014;风险比0.44,95%可信区间0.25~0.79),而两组间其他长期随访期间临床结果差异无统计学意义。
结论:TR进行冠脉三支病变患者的同期介入治疗是安全、可行的,并具有与TF介入治疗相似的手术成功率,具更短的住院时间、更低的出血风险、更低的死亡率,长期疗效不亚于TF介入治疗。
冠状动脉疾病;桡动脉;股动脉;安全性
Methods: A total of 4974 consecutive patients with triple vessel lesion CAD without LM disease who received onestage PCI were enroll in this study. The patients were divided into 2 groups: TR group, n=3856 and TF group, n=1118. The procedural and clinical results were obtained from data base and follow-up study. There were 930 pairs of patients with comparable baseline data obtained from propensity score matching method served as control subjects for both TR and TF groups. The risk diversity between 2 groups was evaluated by Cox’s proportional-hazards model, the cumulative incidences for the safety and efficacy were estimated by Kaplan-Meier method and meanwhile compare by log-rank test.
Results: With propensity score matching, the clinical and angiographic characteristics were similar between 2 groups. TR group had the shorter in-hospital time than TF group (7.49 ± 4.46) days vs (8.63 ± 6.23) days, P<0.0001 and less incidence of bleeding 1.1% vs 2.9%, P<0.003; the other procedural feathers were similar between 2 group. The follow-up study presented that TR group had obviously lower all cause mortality than TF group (1.8% vs 4.2%,
P=0.0014; HR=0.44, 95% CI 0.25-0.79); the other longer term follow-up outcomes were similar between 2 groups.
Conclusion: TR intervention is safe and feasible for treating the patients with triple vessel lesion CAD, the procedural success rate and long term outcomes are similar to TF intervention, while it has shorter in-hospital time, lower risks for bleeding and death.
(Chinese Circulation Journal, 2015,30:311.)
经股动脉(TF)径路是冠状动脉(冠脉)血管成形术常选取的径路,但常导致血管径路并发症增多和住院时间延长[1,2]。因经桡动脉(TR)径路已被证实具有减少出血并发症、术后无需卧床并提高患者舒适度等优点[3-7],在行冠脉介入治疗时[甚至包括急性心肌梗死(AMI)、无保护的左主干病变和老年患者等复杂情况]可以选择TR径路替代标准的TF径路[2,8,9]。然而目前还少见对经TR和TF介入治疗冠脉三支病变住院期间和长期随访期间临床结果的比较研究[10,11]。
1 对象与方法
研究对象:本研究选取了2004-04至2010-10期间我院行冠脉造影确诊为冠脉三支病变并接受经皮冠脉介入治疗(PCI)的连续5 798例患者,评价其住院期间的结果和长期临床结果。冠脉三支病变定义为冠脉三支主要的血管狭窄均大于50%。排除了急诊PCI、分次PCI以及经TR和TF双径路介入治疗的患者后,本研究最终入选了4 974例患者(TR组3 856例,TF组1 118例)。
手术的实施及术后的干预血管径路、介入治疗策略由心脏专科介入医生决定。支架的类型和品牌由术者选择,研究中涉及的支架品牌有:Cypher雷帕霉素洗脱支架(Cordis Europa N.V.,荷兰LJ.Roden),Taxus紫杉醇洗脱支架(Boston scientific,爱尔兰戈尔韦),Firebird雷帕霉素洗脱支架(Microport,中国上海)和Excel雷帕霉素洗脱支架(JW Medical Co.Ltd,中国山东)。
术前所有患者均服用阿司匹林300 mg每日1次,术前至少提前1天服用氯吡格雷300 mg的负荷剂量。术中均予每公斤体重100 U的普通肝素。术后3个月服用阿司匹林300 mg每日1次,后改为100 mg每日1次长期服用。服用氯吡格雷75 mg每日1次,至少1年。
随访资料的采集和主要监测指标:手术成功判定标准为血管造影成功,介入治疗后心肌梗死溶栓治疗临床试验(TIMI)血流3级、目测残余狭窄<30%,且术后未发生住院期间死亡、心肌梗死(MI)或急诊行冠脉旁路移植术(CABG)。评价住院期间的出血事件,并根据所有记录的出血事件特点应用TIMI出血分级标准(严重、轻微) 进行分级[12,13]。
随访数据通过术后第1、3、6、12个月及其后每年一次的门诊或电话随访完成。平均随访时间21个月,主要监测指标包括支架内血栓形成 (肯定、肯定/可能、早期、晚期及极晚期) 、全因死亡率、心肌梗死、靶病变血运重建(TVR)和主要不良心脏事件(MACE,即死亡、心肌梗死和TVR复合发生率)。所有终点均按照学术研究联合会(ARC) 的定义进行界定。

2 结果
2.1 倾向评分匹配前后临床特点、冠状动脉病变特点和处理情况
倾向评分匹配前,TF组患者年龄、女性、既往心肌梗死病史、既往PCI病史、既往CABG病史、糖尿病、高血压、高脂血症、不稳定性心绞痛均显著高于TR组,左心室射血分数、平均病变数量低于TR组,差异均有统计学意义(P均<0.05~0.001)。其余差异无统计学意义(表1)。TF组再狭窄病变、完全闭塞病变、B2-C型病变、开口病变、中重度钙化病变均显著高于TR组,TF组前降支病变及直接支架置入术的患者比例低于TR组,差异均有统计学意义(P均<0.01)。TR组使用6F指引导管大于TF组(P<0.01)。表2

表1 倾向评分匹配前患者临床特点

表2 倾向评分匹配前患者冠状动脉病变特点及处理情况
共有930例TR组患者与930例TF组患者相匹配进入后续统计学分析。相对标准差小于10%。对倾向评分有很好的预测价值(C-statistic值为0.783)和校准能力(Hosmer-Lemeshow检验,P=0.26)。
倾向评分匹配后两组基线资料差异无统计学意义(表3)。在TF组中使用6号指引导管的比例显著低于TR组(6F:82.7%比97.1%,P<0.0001)。表4

表3 倾向评分匹配后患者临床特点

表4 倾向评分匹配后患者冠状动脉病变特点及处理情况
2.2 倾向评分匹配后的住院期间及长期随访期间临床结果
两组患者在住院期间手术成功率、死亡率或心肌梗死的发生率、造影剂用量及X线暴露时间、TIMI严重出血及输血差异无统计学意义(P>0.05)。 TR组比TF组患者住院时间及术后在院时间显著缩短; TIMI轻微出血事件显著降低; PCI术后血红蛋白下降幅度更小,差异均有统计学意义(P均<0.01)。表5
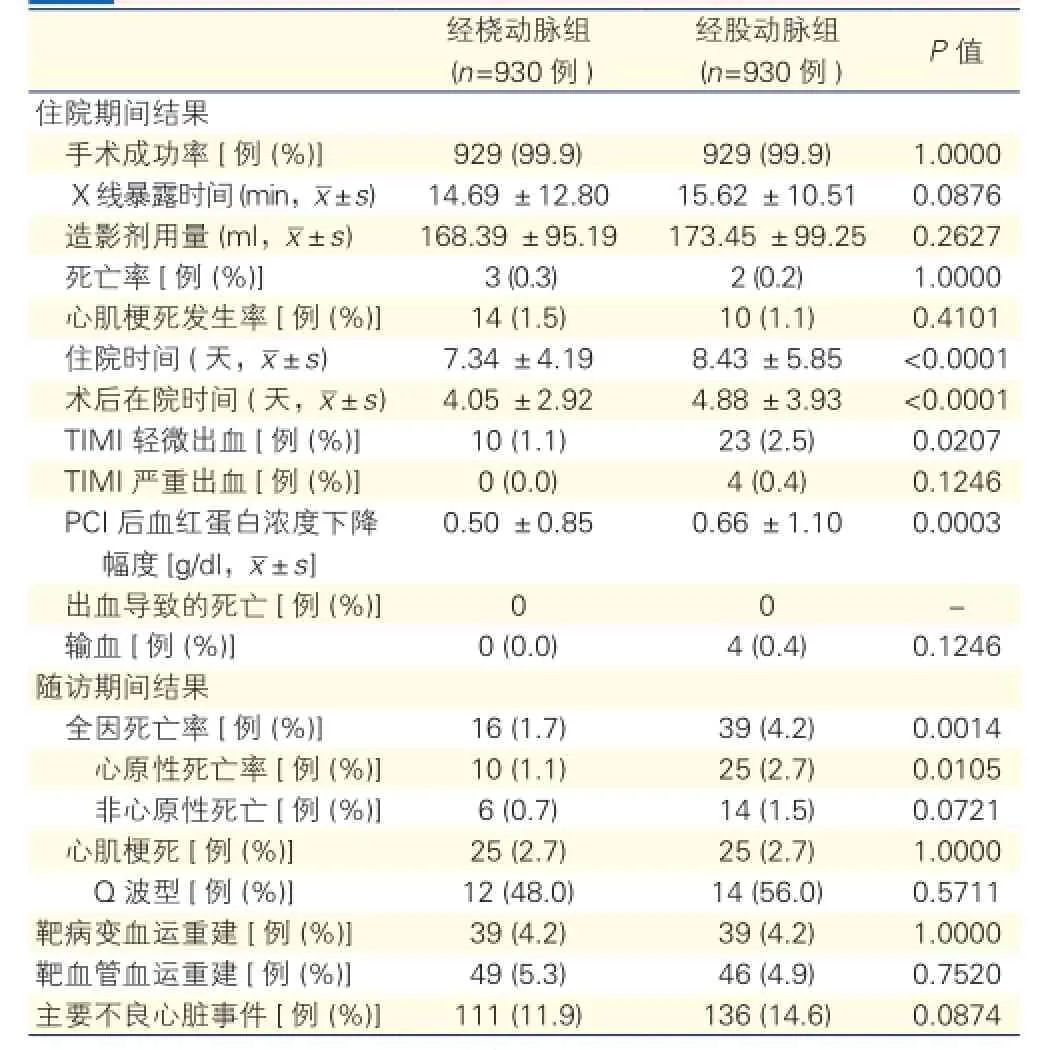
表5 倾向评分匹配后患者住院期间及随访临床结果
本研究进行了15~38个月的临床随访。TR组全因死亡率及心原性死亡率显著低于TF组,差异有统计学意义(P均<0.05~0.01)。其他各项差异无统计学意义(表5)。两组患者肯定的和可能的支架内血栓形成发生率和血栓形成的时间(早期、晚期、极晚期) 差异无统计学差异。表6

表6 倾向评分匹配后患者支架内血栓形成事件累积发生率[例(%)]
倾向评分匹配后校正的临床结果的比较显示,TR组全因死亡风险较TF组显著降低(风险比0.44,95%可信区间0.25~0.79),其他临床事件的风险比在两组间无统计学意义。根据Kaplan-Meier法估计及log-rank检验的结果(图1),也证实了TR组的全因死亡率(2.7%)比TF组(5.9%)显著降低(P=0.0049)。两组间心肌梗死、靶病变(原支架内或支架两端5 mm内的病变)血运重建、靶血管(包括因靶病变以外区域或自身原发病变进展或新形成的病变)血运重建、主要不良心脏事件以及支架内肯定/可能的血栓形成等事件的长期累积发生率没有统计学意义。
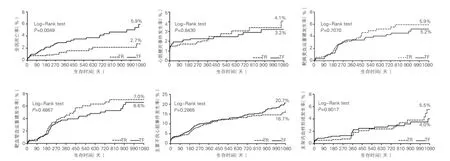
图1 倾向评分匹配后Kaplan-Meier法评价长期随访临床结果
3 讨论
近20年来,随着介入诊治器械制作技术的进步,TR路径行PCI术已逐渐成为首选路径。与TF路径相比,桡动脉入路穿刺处发生出血、血肿、假性动脉瘤并发症相对较低、患者术后无需绝对卧床、制动24 h,且避免了TF穿刺后,长时间的压迫止血
极易引起反射呕吐等不良症状,近十余年该术式得到广泛的推广和普及,目前国内一些医学中心,如我院TR介入治疗(TRI)已成为主要术式。
TRI治疗,随着介入器械的不断发展适应证范围也不断拓展。TRI手术已不仅仅局限于简单冠脉病变,TR处理无保护左主干病变、TR处理慢性闭塞性病变(CTO)病变、TR对急性心肌梗死、分叉病变等均有国内外文献报道[26-29],临床应用中已成为普遍接受的事实。然而目前还少有TR和TF介入治疗冠脉三支病变的住院期间和长期临床结果进行比较研究[10,11]。
从本研究可以看出TR组和TF组比较两组在手术成功率、X线曝露时间、造影剂用量等方面无统计学意义。此外,两组患者术后血肿的发生因程度不同,未纳入统计范畴。桡动脉位置表浅,周围无关节活动,也无肌肉、大血管及静脉伴行,可降低动静脉瘘的发生,且易于压迫,易于止血控制,术后出血并发症与TF组比较明显减少。同时因桡动脉是肌性动脉,交感神经兴奋性高,易发生痉挛,血管穿刺及导管操作难度相对较大,对手术操作者要求较高。目前多主张在血管条件允许的情况下采用TR途径。对于部分患者造影中出现痉挛、过度迂曲,或上肢动脉闭塞的不建议采用TRI治疗。
本研究是目前最大的针对冠脉三支病变患者同期进行介入治疗时TR和TF住院期间及和长期临床结果的观察性队列研究。本研究的主要发现:对于冠状三支病变患者进行同期介入治疗时,TR PCI是安全可行的;TR PCI出血并发症明显减少;TR PCI可缩短住院时间;与TF PCI相比,倾向评分匹配后TR PCI治疗冠脉三支病变患者的死亡率显著降低。尽管两组患者近期及远期临床结果相似,这些发现让我们更有信心通过TR PCI对三支病变同期进行处理。
本研究结果提示TR介入治疗冠脉三支病变是安全可行的。一些随机观察性研究表明与TF相比,TR可减少出血并发症及血液制品的输注[1,4,7,16,17]。与之前的研究结果一致,我们发现对于冠脉三支病变患者,TR 介入治疗可以显著减少出血并发症P=0.0207)及PCI术后血红蛋白的降低(P=0.0003)。TF组中术后出血引起的输血更为常见,尽管两组间比较无统计学差异。较多的出血及血管并发症会从而导致潜在的住院时间延长及住院费用的增加。事实上,本研究表明TR PCI显著缩短了住院时间及术后在院期间。从而减少各种费用[18-21]。
除死亡率外,两组的长期临床结果相似,在靶血管血运重建中已统计包含了再次CABG的发生,两组的靶血管血运重建发生率相似。这一有利的结果可能部分归功于后扩张、高压释放、新成像模式、新设备等技术改进在TR径路时依然可以应用[1,4,22,23]。一些大规模的比较研究已经指出了低死亡率与TR PCI间的联系,可能是因为TR PCI减少了出血和(或)输血的发生所致[4,16,25]。与之类似,本研究发现对于冠脉三支病变的患者,TR组全因死亡率及心原性死亡率显著减低。TR PCI容易止血、血管径路并发症更少、指引导管尺寸更小、血红蛋白下降程度更小使得出血事件减少、死亡率降低。然而,我们需要注意的是有关死亡率的数据是基于一项回顾性、非随机性的研究,其只能推论出一个假说而不是证明这一观点。TR和TF PCI治疗冠脉三支病变死亡率是否存在差异还需要进一步的大规模随机行试验来证明。
研究的局限性:本研究为回顾性非随机化研究,隐藏的混杂因素和其他来源的偏倚不可避免。尽管期望通过倾向评分来校正可观测到的潜在的无法测量的混杂因素,但仍有一些残余的混杂因素的影响无法排除。另外倾向评分匹配可能检验效能降低。因此,未来还需要大规模随机试验来比较经两种通路介入治疗冠脉三支病变的手术和长期临床结果。
[1] Jolly SS, Amlani S, Hamon M, et al. Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: a systematic review and meta-analysis of randomized trials. Am Heart J, 2009, 157: 132-140
[2] Cantor WJ, Puley G, Natarajan MK, et al. Radial versus femoral access for emergent percutaneous coronary intervention with adjunct glycoprotein IIb/IIIa inhibition in acute myocardial infarction—the RADILAMI pilot randomized trial. Am Heart J, 2005, 150: 543-549.
[3] Cooper CJ, EL-Shiekh RA, Cohen DJ, et al. Effect of transradial access on quality of life and cost of cardiac catheterization: a randomized comparison. Am Heart J, 1999, 138: 430-436.
[4] Chase AJ, Fretz EB, Warburton WP, et al. Association of the arterial access site at angioplasty with transfusion and mortality: the M. O. R. T. A. L study (Mortality benefit Of Reduced Transfusion after percutaneous coronary intervention via the Arm or Leg. Heart, 2008, 94: 1019-1025.
[5] Martin B, Dirk B, Wilfried K, et al. HaraldTillmanns, A randomized comparison of transradial versus transfemoral approach for coronary angiography and angioplasty, J Am CardiolIntv, 2009, 2: 1047-1054.
[6] Brueck M, Bandorski D, Kramer W, et al. A randomized comparison of transradial versus transfemoral approach for coronary angiography and angioplasty. J Am Coll Cardio Intv, 2009, 2: 1047-1054.
[7] Rao SV, Ou F, Wang TY, et al. Trends in the prevalence and outcomes of radial and femoral approaches to percutaneous coronary intervention: a report from the National Cardiovascular Data Registry. J Am CollCardiolIntv, 2008, 1: 379-386.
[8] Yuejin Y, David K, Zhan G, et al. Transradial versus transfemoral method of percuatneous coronary revascularization for unprotected left main coronary artery disease: comparison of procedural and late-term outcomes. J Am CollCardiolIntv, 2010, 3: 1035-1042.
[9] Stephan A, Dieter R, Lisa K, et al. Transradial versus transfemoral approach for coronary angiography and intervention in patients above 75 years of age. Cathet Cardio Interv, 2008, 72: 629-635.
[10 ] Matthias T, Neuhauser M, Stephan K, et al. Prognostic impact of previous percutaneous coronary intervention in patients with diabetes mellitus and triple-vessel disease undergoing coronary artery bypass surgery. J Thoracic Durg, 2007, 134: 470-476.
[11] Gijong Y, Youngnam Y, Soonchang H, et al. Comparison of long-term outcome of off-pump coronary artery bypass grafting versus drugeluting stents in triple-vessel coronary artery disease. Am J Cardiol, 2012, 109: 819-823.
[12] Bovill EG, Terrin ML, Stump DC, et al. Hemorrhagic events during therapy with recombinant tissue-type plasminogen activator, heparin, and aspirin for acute myocardial infarction: results of the Thrombolysis In Myocardial Infarction (TIMI), PHASE ii TRIAL. Ann Intern Med, 1991, 115: 256-265.
[13] The GUSTO Investigators. An international randomized trial comparing four thrombolytic strategies for acute myocardial infarction. N Engl J Med, 1993, 329: 673-682.
[14] Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation, 2007, 115: 2344-2351.
[15] D' Agostino, RB Jr. Propensity score methods for bias reduction in the comparison of a treatment to a non-randomized control group. Stat Med, 1998, 17: 2265-281.
[16] Sciahbasi A, Pristipino C, Abrosio G, et al. Arterial access-siterelated outcomes of patients undergoing invasive coronary procedures for acute coronary syndromes(from the ComPaRison of Early Invasive and Conservative Treatment in Patients With Non-ST-ElevatiOn Acute Coronary yndromes(PRESTO-ACS)Vascular Substudy). Am J Cardio, 2009, 103: 796-800.
[17] Hamon M, Rasmussen LH, Manoukian SV, et al. Choice of arterial access site and outcomes in patients with acute coronary syndromes managed with an early invasive strategy: the ACUITY trial. EuroIntervention, 2009, 5: 115-120.
[18] Kugelmass AD, Cohen DJ, Brown PP, et al. Hospital resources consumed in treating complications associated with percutaneous coronary interventions. Am J Cardiol, 2006, 97: 322-327.
[19] Rao SV, Kaul PR, Liao L, et al. Association between bleeding, blood transfusion, and costs among patients with on-ST-segment elevation acute coronary syndromes. Am Heart J, 2008, 155: 369-374.
[20] Mann T, Cowper PA, Peterson ED, et al. Transradial coronary stenting: comparison with femoral access closed with an arterial suture device. Catheter CardiovascInterv, 2000, 49: 150-156.
[21] Roussanov O, Wilson SJ, Henley K, et al. Cost-effectiveness of the radial versus femoral artery approach to diagnostic cardiac catheterization. J Invasive Cardiol, 2007, 19: 349-353.
[22] Park SJ, Kim YH, Park DW, et al. Impact of intravascular ultrasound guidance on long-term mortality in stenting for unprotected left main coronary artery stenosis. Circ CardiovascInterv, 2009, 2: 167-177.
[23] Mauri L, Silbaugh TS, Wolf RE, et al. Long-term clinical outcomes after drug-eluting and bare-metal stenting in massachusetts. Circulation, 2008, 118: 1817-1827.
[24] Schomig A, Dibra A, Windecker S, et al. A meta-analysis of 16 randomized trials of sirolimus-eluting stents versus paclitaxel-eluting stents in patients with coronary artery disease. J Am CollCardiol, 2007, 50: 1378-1380.
[25] Yatskar L, Selzer F, Feit F, et al. Access site hematoma requiring blood transfusion predicts mortality in patients undergoing percutaneous coronary intervention: data from the National Heart, Lung, and Blood Institute Dynamic Registry. Catheter CardiovascInterv, 2007, 69: 961-966.
[26] Cheng CI, Wu CJ, Fang CY, et a1.Feasibility and safety oftransradial stentingfor unprotected left main coronary artery stenoses.Circ J, 2007, 71: 855-861.
[27] Hsueh SK, Hsieh YK, Wa CJ, et a1.Immediate results of percutaneous coronary intervention for unprotected left main coronary artery stenoses: transradial versus transfemoral approach.Chang Gung Med J, 2008, 31: 190-200
[28] Kim JY, Lee SH, Choe HM, et a1.The feasibility ofpercutaneous transradial coronary intervention for chronic total occlusion.Yonsei Med J, 2006, 47: 680-687.
[29] Saito S, Tanaka S, Hiroe Y, et a1.Comparative study on transradial approach VS.transfemoral approach in primary stent implantation for patients with acute myocardial infarction: results of the test for myocardial infarction by prospective unicenter randomization for access sites(TEMPURA)tria1.Catheter Cardiovasc Interv, 2003, 59: 26-33.
[30] 周玉杰, 聂斌. 经桡动脉冠状动脉介入治疗现状和未来. 中国循环杂志, 2009, 24: 81-83.
[31] 杨跃进, 窦克非. 经桡动脉对冠状动脉慢性完全闭塞病变介入治疗的策略及操作技巧. 中国循环杂志, 2008, 32: 310-311.
[32] 刘圣文, 乔树宾, 徐波. 经桡动脉介入治疗冠心病的住院期间疗效和主要不良心 脏事件的预测因素. 中国循环杂志, 2011, 39: 208-211.
Comparison of In-hospital and Long Term Clinical Outcomes Between Trans-radial and Trans-femoral Approaches in Patients of Triple Vessel Lesion CAD With Percutaneous Coronary Intervention
LI Jia, XU Han, DOU Ke-fei, XU Bo, YOU Shi-jie, WU Yong-jian, QIAO Shu-bin, YAN Hong-bing, YANG Yue-jin.
Department of Cardiology, Cardiovascular Institute and Fu Wai Hospital, CAMS and PUMC, Beijing (100037), China
Objectives: To evaluate the safety, feasibility, in-hospital and long-term follow-up period outcomes by trans-radial (TR) approach for treating the patients of triple vessel lesion coronary artery disease (CAD) with one-stage percutaneous coronary intervention (PCI) in comparison with trans-femoral (TF) access.
Coronary artery disease; Radial artery; Femoral artery; safety
2014-11-04)
(编辑:常文静)
100037 北京市, 中国医学科学院 北京协和医学院 国家心血管病中心 阜外心血管病医院 冠心病诊治中心
李佳 主治医师 主要从事心血管内科相关疾病治疗 Email:litdoctorlij@163.com*为共同第一作者 通讯作者:窦克非Email:drdoukefei@sohu.com
R54
A
1000-3614(2015)04-0311-06
10.3969/j.issn.1000-3614.2015.04.003
猜你喜欢
昆明医科大学学报(2021年12期)2021-12-30
实用心电学杂志(2021年5期)2021-10-26
昆明医科大学学报(2021年3期)2021-07-22
世界最新医学信息文摘(2021年12期)2021-06-09
探索科学(学术版)(2020年10期)2021-01-13
保健与生活(2020年24期)2020-12-23
铁道通信信号(2018年7期)2018-08-29
中国介入心脏病学杂志(2018年2期)2018-03-21
中国介入心脏病学杂志(2017年10期)2017-11-15
中华心脏与心律电子杂志(2017年2期)2017-10-20
