
Effect of cold weather on carotid artery stenosis and occlusion: A retrospective observational study
2022-04-12 10:54HamissouMoussaMamanRoufaiJunYangGuangFuSongFuYiYang
Journal of Acute Disease 2022年2期
Hamissou Moussa Maman Roufai, Jun Yang, Guang-Fu Song, Fu-Yi Yang
Department of Neurosurgery, First Affiliated Hospital of Jiamusi University, Jiamusi City, Heilongjiang Province, China
ABSTRACT Objective: To investigate the effect of cold weather on carotid artery stenosis and occlusion.Methods: We conducted a retrospective observational study, in which 145 patients with carotid artery stenosis and occlusion were enrolled [115 men and 30 women; the mean age was 61.08 years (95% CI 59.27-62.88)].Patients were divided into the lowtemperature group (n=98) (≤12 ℃) and the non-low temperature group (n=47) (>12 ℃).Clinical characteristics, blood pressure, National Institutes of Health Stroke Scale (NIHSS), blood fat, and blood viscositys were compared between the two groups.Correlation between NIHSS and mean daily temperature was analyzed.Results: There was no significant difference in the systolic and diastolic blood pressure between the two groups (P>0.05).The NIHSS score was slightly higher in the non-low temperature group compared to that of the low-temperature group (U=2 984, P<0.01).Glycemia, cholesterol level, prothrombin time, fibrinogen, and International Normalized Ratio did not show any significant difference (P>0.05).Correlation analysis showed a very low positive and statistically significant correlation between ambient temperature and NIHSS score (r=0.18, P=0.029).Conclusion: Cold weather does not impact blood pressure, blood cholesterol, and coagulation factors of patients with carotid artery stenosis and occlusion.The neurological deficit is more severe in the non-low ambient temperature group.A potential relationship exists between ambient temperature and the level of neurological impairment.
KEYWORDS: Cold weather; Carotid artery stenosis; Carotid artery occlusion; Ischemic stroke; Seasonal variation
1.Introduction
Low ambient temperature is related to high incidence and mortality of stroke.Many researchers reported increased incidence and mortality of stroke during the winter season[1-3].Even though few studies demonstrated that both low and high ambient temperature were associated with increased stroke mortality[4-6], more countries worldwide reported the tendency of high mortality of stroke during winter[7-10].
The fundamental mechanism underlying the high incidence and mortality of stroke during the winter is still not well elucidated.Many studies in the cardiovascular field tried to explain the relationship between low ambient temperature and cardiovascular disease.Some hypotheses proposed that ambient temperature changes might affect blood pressure, cholesterol levels, blood viscosity, and coagulation, which were confirmed by Yu et al.in 2020 and found that each 10 ℃ decrease in outdoor temperature would reduce 6.7 mmHg in systolic blood pressure and 2.1 mmHg in diastolic blood pressure when the outdoor temperature higher than 5 ℃[11].Sartini et al.in 2016 explored the relationship between outdoor temperature and cardiovascular disease risk factors in older patients.They showed that lower outdoor temperature induced an adverse effect on cholesterol, blood pressure, inflammatory markers, and vitamin D[12].Additionally, it demonstrated low ambient temperature-induced atherosclerotic plaque growth and instability[13,14].However, Guinea et al.in 2008 showed that an increase in corporal temperature could promote atherosclerotic plaque rupture[15], and Madaniyazi et al.reported that lower and higher ambient temperature would affect cholesterol levels[16].
Recently, many studies have been conducted in the cerebrovascular field to assess the relationship between low temperature and stroke occurrence but most of them are epidemiological[2,17-19]; few tried to explain the pathophysiological mechanism of higher incidence and mortality of stroke during the winter[1,20,21].
Jiamusi is located in the humid climate area of the middle temperate zone, belonging to the continental monsoon climate.The city’s annual average temperature is about 3 ℃.The winter is long, while the summer is short.The temperature rises in spring, with strong wind and is drought-prone.The summer is warm and rainy, and the climate is humid.In autumn, the weather is pleasant, and the temperature drops rapidly.Winter is long, cold, and dry.The average temperature is above 0 ℃ in 7 months (from April to October).
This study investigated the effect of cold weather on carotid artery stenosis and occlusion.We hypothesized that cold weather might promote high blood pressure, high blood cholesterol, and blood viscosity in a patient with carotid artery stenosis and occlusion.We also hypothesized that carotid artery stenosis and occlusion may be more likely to occur in cold weather, and the neurological impairment can be more severe.
2.Patients and methods
2.1.Study design
We conducted a retrospective observational study in the Department of Neurosurgery and Neurology of the First Affiliated Hospital of Jiamusi University from December 2019 to June 2021.
2.2.Patients selection
We included all patients with carotid artery stenosis or occlusion who were over 18 years and admitted in the Department of Neurosurgery and Neurology.The diagnosis was based on carotid Duplex ultrasounds, computed tomographic angiography, magnetic resonance angiography, or digital subtracted angiography.
We excluded all patients with carotid stenosis caused by fibromuscular dysplasia, trauma, and carotid dissection.
Based on the previous study[13,20], we chose the cutoff of 12 ℃ for defining low ambient temperature (the average daily temperature ≤12 ℃) and non-low ambient temperature (the average daily temperature> 12 ℃).
One hundred and forty-five (145) patients with carotid artery stenosis and occlusion were included and divided into the lowtemperature group (n=98) and the non-low temperature group (n=47) (Figure 1).

Figure 1.The study flowchart.
2.3.Meteorological data
Jiamusi’s online historical weather data website (https://m.tianqi.com/lishi/jiamusi/index.html) provided meteorological data, including the maximum daily temperature and minimum daily temperature.We calculated the mean daily temperature of the hospital admission day of all included patients by adding the highest daily temperature and the lowest daily temperature, then the mean value was obtained.
2.4.Data collection
We collected data throughout a standardized form.The studied variables included blood pressure, National Institutes of Health Stroke Scale (NIHSS), degree of stenosis, cholesterol, and coagulation parameters.We obtained the demographic and clinical records of the patients by reviewing the medical records.Immediately after admission, a detailed physical examination was performed, and all clinical parameters were registered.For our study, we considered the blood pressure recorded at the admission time before using any medication, and the laboratory examinations performed within the 8 h after admission.The NIHSS score was used to assess the neurological impairment and was performed repeatedly during the patient’s hospital stay.The degree of stenosis was as mild<50%, moderate 50% to 69%, significant 70% to 89%, severe 90% to 99%, and complete occlusion 100%.Blood samples analyses were performed within 24 h of hospital admission for blood glucose, cholesterol high-density lipoprotein, low-density lipoprotein, total cholesterol, very-low-density lipoprotein, triglyceride, plasma fibrinogen, prothrombin time, and International Normalized Ratio (INR).
2.5.Ethical approval
The Ethics Committee of the First Affiliated Hospital of Jiamusi University approved this study (decision number: 2020-11-24).The study was conducted in accordance with the Declaration of Helsinki.
2.6.Statistical analysis
SPSS (Statistical Package for the Social Sciences) software version 26 was used to perform statistical analysis.As the data did not follow a normal distribution, the variables were expressed by median and interquartile, and the Mann-Whitney test was used to compare the continuous and scale variables between the two groups.The Chisquare test was used for categorical and nominal variables (history of hypertension, diabetes, smoking, alcohol consumption, coronary heart disease, degree of stenosis, and the principal chief complaint).These data were described using frequency and percentage.Besides, Spearman’s rank correlation analysis was used to investigate the relationship between ambient temperature and NIHSS score.The significant level of this study was set at α=0.05.
3.Results
From December 2019 to June 2021, 145 patients with carotid artery stenosis and occlusion were admitted to the Department of Neurosurgery and Neurology of the First affiliated Hospital of Jiamusi University.There were 115 men and 30 women (Figure 1); the mean age was 61.08 (95% CI 59.27-62.88).They were divided into the low-temperature group (n=98 cases) and the non-low temperature (n=47 cases).There were no significant differences in age (χ2=40.79, P=0.56) and gender (χ2=2.05, P=0.15) between the two groups.
3.1.Clinical characteristics
There was no significant difference in hypertension, diabetes, or coronary heart disease, and no significant difference in current smoking and drinking (P>0.05).The common chief complaint in both groups was numbness or weakness, and no significant difference was found between the two groups (P>0.05).The proportion of the respective degree of stenosis, significant stenosis, severe stenosis, and complete occlusion was slightly higher in the low-temperature group, but the difference was not significantly different (χ2=5.16, P=0.20).At the same time, proportion of mild and moderate stenosis was higher in the non-low temperature group, but these differences are not statistically significant as well (P>0.05) (Table 1).
3.2.Risk factors, stroke severity, and coagulation factors
There was no significant difference in the systolic and diastolic blood pressure between the two groups.The NIHSS score was higher in the non-low temperature group (P<0.05).Glycemia, cholesterol parameters, prothrombin time, fibrinogen, and INR did not show any significant difference (P>0.05).All the results were shown in Table 2.

Table 1.Comparison of the clinical characteristics between the low-temperature group and the non-low temperature group.
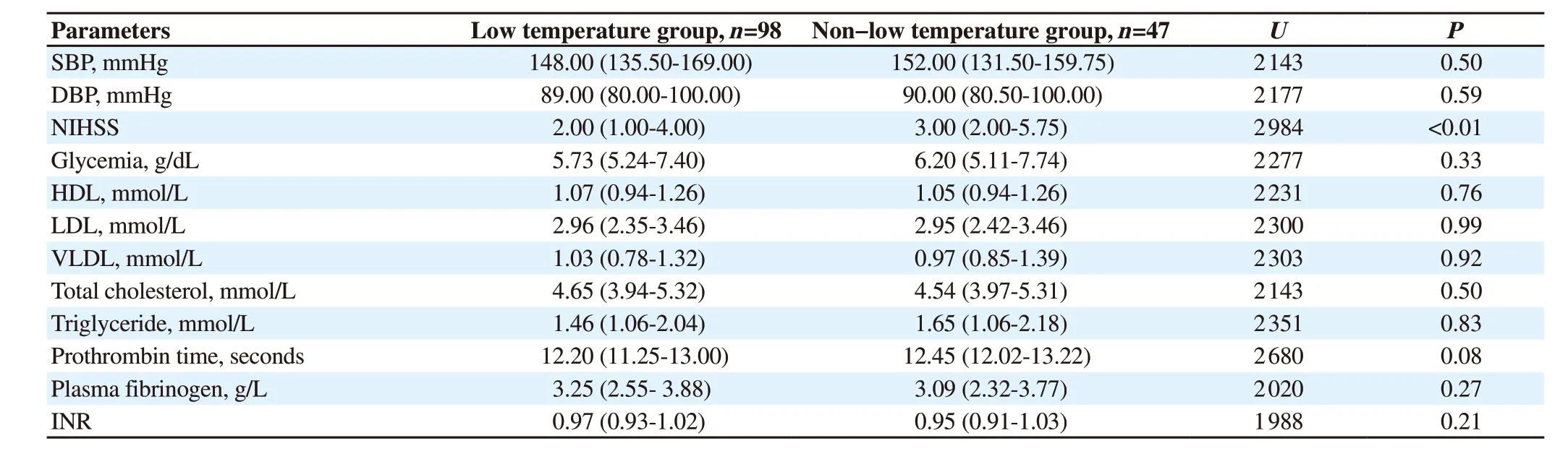
Table 2.Comparison of blood pressure, NIHSS, blood fat, and blood viscosity parameters between the low temperature and the non-low temperature groups.
3.3.Relationship between ambient temperature and NIHSS score
Spearman’s rank-order correlation was run to examine the relationship between ambient temperature and level of neurological impairment (NIHSS).There was a very weak positive and significant relationship between ambient temperature and NIHSS score (r=0.18, P=0.029).
4.Discussion
The findings from this study indicate that there is no difference in blood pressure for the low-temperature group compared with the nonlow temperature group.The possible explanation is that more than 60% of the patient in both groups have a medical history of hypertension.Similarly, Ogata et al.in Japan evaluated the seasonal variation of frequency of acute ischemic stroke in 12 669 patients, and no differences in blood pressure were observed across the four seasons[22].The same findings were reported by Toyoda et al.in the five-year single-center observational study, including 2 965 patients to evaluate the seasonal variation in stroke severity and outcomes[23].In contrast, Chen et al., assessed the effect of winter temperature on a patient with ischemic stroke, and found a significant difference in blood pressure between the low-temperature group and non-low temperature group.The blood pressure seems to be higher during the winter when the temperature is <13 ℃[20].Several reasons may explain the differences among studies.A single take of blood pressure during admission when the symptoms are acute may not be enough to determine the actual effect of low temperature on the blood pressure on a patient with carotid artery stenosis and occlusion.Furthermore, the exposition time, the use of inside heating, and other precautions against cold weather vary from person to person and from area to area can be a factor of differences among studies.
Our study indicates that the neurological impairment is more severe when the temperature is higher than 12 ℃.The NIHSS score in the non-low temperature group is slightly higher than in the lowtemperature group.Few studies investigated the relationship between low temperature and the level of stroke severity, and different results are reported.Ogata et al.enrolled 12 669 patients to investigate the variation in ischemic stroke frequency in Japan, and the result showed no difference in NIHSS score of different seasons[22].Similarly, Alghamdi et al.reported the same effect in a single-center study evaluating the stroke seasonality and weather association[24].Differently, Liu et al.said more severe stroke in spring and winter than fall and summer when assessing the seasonal variation of admission severity and outcomes in patients with ischemic stroke[25].
In contrast, Chen et al.reported more severe stroke when the temperature is <13 ℃[20].The pathophysiological mechanism of low temperature related to stroke severity remains unclear.The suggested mechanism of vasoconstriction may explain an increase in blood pressure and then the high frequency of stroke during the winter period[26].
Furthermore, cold exposure was previously related to atherosclerotic plaque growth and instability due to increased plasma low-density lipoprotein[13,14].This finding can give a consistent explanation of previous studies on stroke occurrence in the winter period.Many authors reported a high stroke incidence and mortality during spring and winter[25,27].
Our study has some limitations.First, this is a retrospective cohort study, which means all the data were obtained through patients’ medical records.There is a possibility of missing some cases and data on several variables.Furthermore, we considered the data of the first clinical record at the admission time and within 8 h after admission for laboratory examinations.Some symptoms or values may be changed before admission.Second, we collected the weather data through a single station, not a single-person exposition.The cold protection tools such as inside heating wearing cold clothes are not considered.We did not include air pollution and other toxicological factors.Third, this is a single-center study.We have another hospital in the city.That means our study did not include all the carotid artery stenosis and occlusion patients during the corresponding period.Moreover, the time range is short that cannot be generalized to the whole of Jiamusi city.
To sum up, this study aimed to investigate the effect of cold weather on carotid artery stenosis and occlusion.The result indicates that neither weather impacts blood pressure, blood cholesterol, and coagulation factors for patients with carotid artery stenosis and occlusion.Further findings showed that the neurological deficit is more severe in the nonlow ambient temperature.However, a potential relationship exists between ambient temperature and the level of neurological impairment.Even though this correlation is shallow in our study, full consideration needs to be given to future studies.
Conflict of interest statement
The authors report no conflict of interest.
Authors’ contributions
H.M.M.R.: Data acquisition, statistical analysis, literature search, manuscript preparation; J.Y.: Design, manuscript editing; G.F.S.: Data acquisition, literature search, F.Y.Y.: Supervised the project and reviewed the manuscript.
 Journal of Acute Disease2022年2期
Journal of Acute Disease2022年2期
- Journal of Acute Disease的其它文章
- Electrocardiographic abnormalities in prevalent infections in tropical regions: A scoping review
- Goal-directed fluid therapy in gastrointestinal cancer surgery: A prospective randomized study
- Comparative study on effects of dexmedetomidine and dexamethasone on the incidence of postoperative nausea and vomiting in patients undergoing laparoscopic surgery
- Body mass index and COVID-19 outcomes: A retrospective crosssectional study at a tertiary care center in India
- Mortality characteristics during the two waves of COVID-19 in India: A retrospective observational study
- An alveolate kidney: A case report of emphysema pyelonephritis