
Neuromyelitis optica spectrum disorders and anti-myelin oligodendrocyte glycoprotein positive optic neuropathies
2022-07-30 10:03PatrickMurtaghAmyComanKirkStephensonMariaGaughanDavidRyanGraemeMcNeillChristopherMcGuiganLorraineCassidy
INTRODUCTION
The authors found that presenting and final VA was not be correlated with RNFL or GCL. With regards to GCL, an average reduction of 2.92 and 7.75 μm was seen in the MOG and AQP4 group respectively. These are extremely modest differences and negligible when the standard error of the OCT machine is taken in account. The RNFL analysis showed a reduction of 58.75 μm in the MOG group as opposed to only 10.5 μm in the AQP4 group. However, this is not an indication of worsening disease but is in keeping with the predominance of OHN swelling in the MOG cohort. This swelling resides with time and is in keeping with the observed reduction in RNFL thickness. Therefore, the authors suggest that analysis of the GCL layer is a more accurate representation of nerve damage as opposed to RNFL, especially in the acute phase of the disease. Waiting 3mo to accurately interpret RNFL would be more appropriate
. RNFL may be used to assess subtle swelling of the nerve and to assess change in chronic disease.OCT is unquestionably finding its foothold in the monitoring of optic nerve disease, where it offers an excellent objective numerical interpretation of inner retinal layers. Loss of these unmyelinated axons is postulated to be secondary to an antegrade process
.
Optic Nerve Head Assessment Optic nerve head assessment is a fundamental aspect of every ocular exam and it is crucial when it comes to the assessment of optic neuropathies as the appearance of the nerve can give crucial hints with respect to aetiology of the disease. Similar topographic changes can appear in chronic or late-stage disease
and therefore it is essential that the disc is assessed at presentation with baseline fundal disc photos taken for comparison with its appearance in follow up visits.
Disease Course As previously stated, 2 of the 12 patients(16.67%) in the MOG cohort and 2 of the 4 patients (50%) in AQP4 cohort the had bilateral involvement at presentation.With regards number of relapses, 5 patients in the MOG cohort had a relapsing course (average of 1.6 relapses, range 1-3)while the remining 7 patients had a single attack (monophasic course) at the time of writing. Two of the patients (60%)who had a recurrent course had sequential progression to the contralateral eye. In the AQP4 group, 2 of the 4 patients(50%) had bilateral involvement at presentation. Three of the 4 patients (75%) had a recurrent course (average of 3 relapses,range 1-7) and 1 of these patients had sequential progression with multiple relapses. The remaining one patient had a monophasic course.
ON seen in MOG positive cases tend to have atypical findings.The 80% patients of those with MOG positive ON tend to have moderate to severe disc oedema
. Patients tend to have recurrent and bilateral attacks of ON
. These patients tend to be highly steroid responsive and can prove to be steroid dependant
.
2)将电熔套管从包装袋中取出,并检查确认配件内壁是干净的。如有需要,可使用酒精擦拭纸擦拭电熔套管内壁,在开始焊接工艺前,确保清洁后的电熔套管内壁是完全干燥。
In contrast to typical ON, high dose intravenous glucocorticoids are recommended are at initial presentation in MOG and anti-Aquaporin 4 (AQP4) positive cases of ON
. Guidelines for treatment have proved difficult to establish due to the low number of patients and therefore the absence of randomised controlled clinical trials.
To describe all cases of anti-MOG antibody positive and AQP4 antibody positive ON that have presented to a specialist ophthalmology quaternary referral centre. This will consist of demographic data, clinical characteristics, ancillary tests [optical coherence tomography (OCT), perimetry and neuroimaging] and treatment/outcome.
SUBJECTS AND METHODS
Ethical Approval This study was a retrospective review and was conducted in accordance with the Declaration of Helsinki and the Irish Data Protection Act. The protocol of the study adhered to the tenets of the Declaration of Helsinki. This study adheres to the legal requirements of the General Data Protection Regulation (GDPR, articles 6 and 9).
新中式建筑以传统文化理念的基础,将我国传统文化的元素通过现代艺术形式来表达出来,不但符合我国民众切实的生活所需,又不落后于当前国内外主流审美理念,属于一种具备独特艺术方式并运用现代审美观念来塑造的具有我国东方风貌的艺术形态。岭南建筑多轻巧趣致,建筑与环境自然融合。本项目吸取两者特点,力求塑造出融合时尚不失古典的岭南新中式建筑风格。
Visual Field Testing Table 5 depicts the visual fields findings associated with each patient in both cohorts and the change in each. Of the MOG cohort, 5 of the 12 patients (41.67%) had generalised visual field depression or an enlarged blind spot(Figure 3). Five of the 12 (41.67%) fields demonstrated an improvement, 5 fields were unchanged from the baseline and 2 (16.67%) demonstrating deterioration in the follow up period. One field in the AQP4 (25%) group showed an improvement from baseline to final while the others remained unchanged.
A cross-sectional single-centre retrospective case series consisting of 16 patients including 12 anti-MOG positive patients, and 4 anti-AQP4 positive patients. Inclusion criteria consisted of all patients who had a positive anti-MOG or positive anti-AQP4 blood result for investigation of a unilateral or bilateral ON who attended the Royal Victoria Eye and Ear Hospital, Dublin, Ireland. Exclusion criteria consisted of patients with negative blood markers for the autoantibodies.There was no exclusion based on age or pre-existing comorbidity.At the initial and each follow up consultation the following parameters were recorded; visual acuity (VA) in logarithm of the minimum angle of resolution (logMAR), colour vision(Ishihara pseudoisochromatic testing), presence/absence of a relative afferent pupillary defect (RAPD), slit lamp biomicroscopy with optic nerve assessment, kinetic visual fields (Octopus Visual Field, Haag-Streit, Switzerland), OCT(Cirrus 5000, Carl Zeiss, Meditec, Dublin, CA, USA) analysis of the macula, ganglion cell layer (GCL) and the retinal nerve fibre layer (RNFL). Each of the patients had magnetic resonance imaging (MRI) scanning of the brain and optic nerves with gadolinium contrast. Colour vision was assessed using 14 of the 38 Ishihara plates and graded as mild (10-14/14), moderate (6-10/14) or severe (0-5/14) depending on number of plates correctly identified as outlined in parentheses.RAPD was assessed for its presence or absence and graded from 0 to 3 in terms of increasing severity
. Red desaturation was assessed using a red hat pin on a white background and participants were asked to compare colour intensity between each eye
.
3k 1H NMR(CDCl3) δ:9.48(d,J=5.1,1 H),8.46-8.44(m,1 H),8.05(d,J=5.1,1 H),7.94-7.87(m,2 H),7.75-7.42(m,4 H),7.40-7.38(m,2 H).
理解是描述对象的特征和由来,阐述此对象与相关对象之间的区别和联系,是分析问题和解决问题的基础,是创建数学思维的前提,是学习数学的根基,是为生活生产服务的源泉。理解是学生学习相关课程内容的背景,既有利于帮助学生理解相关内容,也促进其将所学知识运用于解决问题的过程中,无疑有利于提高学生的应用数学的意识和能力。
Statistical Analysis Data was collated and analysed using the statistical package STATA (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP).A statistically significant result was defined as
<0.05. Best corrected VA was recorded in the patient’s medical notes in Snellen format in metres which was subsequently converted to the logMAR for the purpose of statistical analysis. A VA of count fingers (CF), hand motion (HM), perception of light(PL) and no perception of light (NPL) were denoted 2.1, 2.4,2.7, and 3.0 on the logMAR scale, respectively.
RESULTS
Baseline Characteristics A total of 16 patients were include in the study. This consisted of 12 (75%) anti-MOG positive ON patients and 4 (25%) anti-AQP4 positive patients. These 16 patients comprised all recorded cases of antibody positive ON that had attended the Royal Victoria Ear and Ear Hospital.Clinical characteristics of the anti-MOG cohort are seen in Table 1 and the anti-AQP4 cohort are seen in Table 2. The average length of the follow up was 16.5mo (range 2 to 41mo)and 47mo (range 2 to 131mo) for the MOG and AQP4 groups,respectively. Female to male ratio was 7:5 in the MOG group and 1:1 in the AQP4 group. Average age of onset in the MOG group was 29.2y with a range of 10 to 61y, while in the AQP4 group the average age was 42y (range 18-55y). Presenting complaint was blurring of vision in 10 of 12 of the MOG group (83.33%). The remaining 2 patients had pain as their presenting symptom (16.67%). In the AQP4 group, 3 out of the 4 patients (75%) experienced a decrease in vision while the remaining one patient had horizontal diplopia. Pain was a feature of all but one of the anti-MOG cohort (91.67%), either retrobulbar (27.27%) or more commonly on eye movement(72.73%). Interestingly, all the patients in the AQP4 cohort(100%) reported an absence of pain.
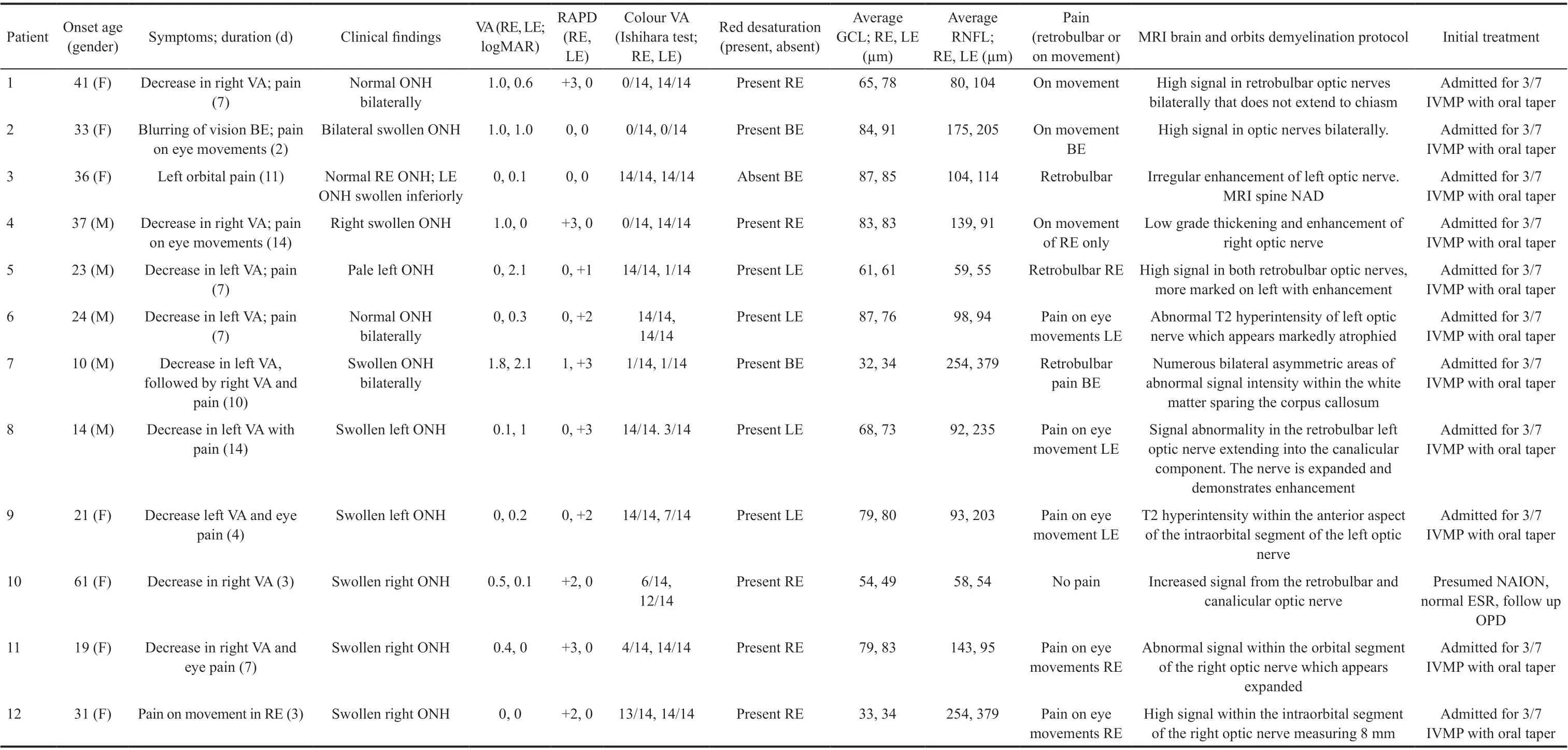
Ocular Findings With regards the affected eye in the MOG group, 5 were right eyes, 5 were left eyes and 2 of the patients had bilateral involvement giving us a total of 14 eyes available for analysis. There were 6 affected eyes in the AQP4 group comprising of 2 left eyes and 2 bilateral. The 11 of 14(78.57%) eyes in the MOG group had visible swollen optic nerve heads (ONH), 2 (14.29%) had normal appearing ONH and the remaining 1 (7.14%) had a pale ONH on presentation.In the AQP4 group, 3 out of the 6 (50%) eyes had either normal or pale appearing ONH and none had a swollen ONH.The presence or absence of an RAPD was also assessed at presentation to the ophthalmic emergency department. Of the MOG group, 11 of the 14 eyes (78.57%) had a RAPD. The presence of an RAPD in the AQP4 group was less with only 2 of the 6 (33.33%) eyes displaying one. The presence of a colour vision defect was also assessed. This was categorised as mild, moderate, or severe as outlined in the methods section.Of the 14 eyes in the MOG cohort, 12 (85.71%) had a colour vision defect. Of these, 9 (75%) were severe, 2 (16.67%)were moderate and 1 (8.33%) was mild. In the AQP4 group,a colour deficiency was observed in 4 of the 6 eyes (66.67%),all 4 being severe in nature. The presence of red desaturation was also assessed in a binary fashion. It was present in all but one eye in the MOG group (92.86%). Only 5 eyes in the AQP4 group were examinable as one eye was NPL, and 3 of the 5 eyes (60%) had this subjective finding.
Visual Acuity and Optical Coherence Tomography Findings Tables 3 and 4 outline initial and final VA in logMAR units, initial and final average GCL and RNFL thickness and the respective change in each for both groups.Only the records for the involved eye were taken for analysis and if both eyes were affected then the data for the more affected eye was utilised. The average presenting logMAR VA in the MOG group was 0.82 (range 0-2.1) while in the AQP4 group it was 1.475 (range 0-3). At last review, the average improvement in VA in the MOG group was -0.66 (range -2.1 to +0.1) and in the AQP4 group was -0.05 (range -0.3 to +0.1).With regards GCL analysis (Figure 1), a modest decrease in thickness was seen in both groups with an average reduction of 2.92 and 7.75 μm in the MOG and AQP4 respectively. The retinal nerve fibre thickness analysis (Figure 2) displayed a greater reduction in thickness, especially in the MOG cohort with an average reduction of 58.75 μm in this group as opposed to only 10.5 μm in the AQP4 group. We examined the correlation between GCL thickness and VA at presentation and as a determinant of final visual outcome in the MOG group. There was no statistically significant correlation(Pearson correlation) between GCL thickness and presenting and final VA [
(10)=0.081,
=0.08 and
(10)=0.089,
=0.34respectively]. The same statistical analysis was performed for the correlation between RNFL and VA and similar outcomes were observed [
(10)=0.04,
=0.22 and
(10)=0.09,
=0.04].In the AQP4 group, moderate correlation was observed between GCL thickness and presenting VA [
(2)=0.61,
=0.42], but this result was not statistically significant. No correlation was seen for initial RNFL thickness and final visual outcome in this group either [
(2)=0.19,
=0.38].




本文首先采用毫秒激光进行打孔实验,利用高速摄影术捕捉打孔过程,得到气化和熔融物的产生及熔融的喷溅情况,研究熔融物的喷溅轨迹和速率。然后依据实验建立模型,利用数值模拟技术模拟研究激光打孔过程熔融物的喷溅情况。最后将两者结果进行比较,证明数值模型的正确性,得到喷溅过程的基本规律。
Visual Acuity and Optical Coherence Tomography Findings Reduction in VA is a hallmark feature in optic nerve disease and the main reason why these patients attend the ophthalmic emergency department as their primary referral source. 81.25%of all eyes (13/16) had a reduction in their VA at presentation.The average presenting logMAR VA in the MOG group was 0.82 as opposed to the AQP4 group whose average VA was 0.655 units worse at 1.475. The average VA in the AQP4 group is compounded by the fact that 1 patient (25%) had a perfect presenting VA of 0 logMAR units. Interestingly, even though the AQP4 group had the greater scope for improvement in vision, it was the MOG group that achieved this (improvement of 0.66 units for the MOG group as opposed to just 0.05 units for the AQP4). If we define long term visual disability as 0.3 logMAR or greater (threshold for driving), all but one of the eyes in the MOG group achieved this (92.86%) as opposed to just 1 eye (25%) in the AQP4 group. These findings are in keeping with what is in the literature where anti-AQP4 positive patients tend to have more severe visual disability
.



Treatment and Maintenance Therapy All patients were treated as inpatients for 3 to 5d of 500 mg twice daily dosing of intravenous methylprednisolone at presentation. Current immunosuppressant therapy, if any, is outlined in Table 6. In the MOG group, azathioprine was the maintenance medication of choice with 5 of the 12 (41.67%) patients receiving it.Two patients were on methotrexate (16.67%), 1 was taking mycophenolate mofetil (8.33%) and 3 of the remaining 4(33.33%; 1 of which was pregnant) were on no maintenance therapy. The final patient was placed on rituximab, underwent plasma exchange and intravenous immunoglobulins (IVIG)and maintenance low dose steroid. In the AQP4 group, two of the patients (50%) were on low dose prednisolone and of the other two, one was taking azathioprine and the other methotrexate to control disease relapse.
As the name of the disease suggest, NMO is defined by both a myelitis and an ON
. The disease has a predilection for both the optic nerves and the spinal cord, and the lesions commonly spare the brain in the early stages
. Patients who have an ON associated with NMO tend to have an acute profound vision loss associated with disc swelling
. However, they may also develop optic nerve atrophy and cavitation akin to glaucomatous optic nerve change in severe cases
. The cavitation is postulated to be secondary to a demyelination associated necrosis of the optic nerve head. The episodes of ON may be recurrent and simultaneously bilateral
causing progressive optic atrophy with cumulative inflammatory damage.



DISCUSSION
Antibody positive optic neuropathies are uncommon. The limited number of seropositive patients available for analysis in our quaternary centre cohort is indicative of this. The female predominance usually seen with these diseases was evident in our sample with an overall female to male ratio of 9:7.
Radiological Findings All but one of the patients in the anti-MOG cohort had sparing of brain involvement (91.67%).All had optic nerve abnormalities observed on MRI imaging(Figure 4). Two (16.67%) of the patients had enhancement in the affected nerve and in the contralateral clinically unaffected nerve. In the AQP4 group, 2 (50%) of the patients had optic nerve enhancement on MRI, one had no evidence of optic neuritis and the final patient had evidence of chiasmitis (Figure 5;Signal abnormality on T2 weighted imaging and uptake with gadolinium).
胶州大白菜通过针对经销商进行单一性供应,使用不同包装,满足了不同的需求制定差异化价格定位,品牌产品价格常年处于市场稳定状态,逐步实现了稳定的供销和利润链条关系,减少了产品的流通环节,且胶州市交通便利,减少了损耗,降低了成本。
(2)断层。矿区内共发现断层5条,其中落差≥100 m的断层3条;落差50~100 m的断层2条。5条断层中,正断层2条,逆断层3条。钻孔揭穿4个断层点,其中1个有漏水现象,其余简易水文观测变化正常。F3、F4、F5断层据部分钻孔揭露未发现漏水现象,富水性以及导水性中等,但在矿床开采后水文地质条件发生变化,人工采矿裂隙大量出现,可能连通含煤地层中的含水层、地表水以及下伏茅口组强含水层,加之以后的矿床开采中,改变了断层带附近应力场和地下水的天然流畅,地表水、地下水更可能沿断裂带进入矿井,起充水和导水作用。
Neuromyelitis optica (NMO; previously known as Devic’s disease) and anti-myelin oligodendrocyte glycoprotein (MOG) optic neuropathy are antibody mediated demyelinating diseases that primarily affect the optic nerves and spinal column and therefore can lead to profound vision and mobility impairment
. They are distinct clinical entities from other demyelinating diseases such as “typical optic neuritis (ON)” and multiple sclerosis (MS; the most common demyelinating disease) and this distinction is important, as these antibody mediated optic neuropathies tend to have more severe presentations, atypical signs and symptoms,recurrent attacks of disease (including simultaneously bilateral or sequential optic neuritis), and they tend to respond well to immunosuppressive therapy and may require long term treatment
. These diseases have a predilection for the optic nerves and visual loss due to ON is often the presenting feature of the disease.
传统的考试主要考核学生的基础知识点掌握情况,题型主要包括以名词解释、填空题、选择题及简答题。本研究依然采用传统的书面考试,但在题型方面做了调整,包括选择题及病例分析题,学生只有对所学知识深入理解、综合分析才能给出正确答案,重点考察学生的临床思维能力。研究结果显示,与传统的教学模式相比,整合医学教学模式对学生考试总成绩及病例分析题成绩均有明显的提升。调查问卷的分析结果表明,整合医学教学模式有利于学生学习动机、自主学习能力的提升,更有助于学生分析解决临床实际问题及临床思维综合运用能力的提高,同时这种教学模式得到学生的普遍认可。
Differentiating from Ischaemic Optic Neuropathies The average age of onset of disease was 29.2y in the MOG group and 42y in the AQP4 group. It is known that that these antibody positive diseases can occur at any age
whereas multiple sclerosis and typical optic neuritis tend to have a younger age of onset usually between 18 and 50y with an average of 32
.One patient in our MOG cohort and two in our AQP4 court were over the age of 50 at their initial presentation. Of these 3 patients, 2 were assumed to have ischaemic optic neuritis(ION) because of their age. In this age group it is imperative to out rule an arteritic cause, as this is a preventable potentially bilaterally blinding condition, and therefore any patient over 50 should have an erythrocyte sedimentation rate (ESR)and c-reactive protein (CRP) undertaken in the ophthalmic emergency department. It can be difficult to differentiate ION from atypical ON in this age bracket. Both anti-MOG positive ON and non arteritic ischemic optic neuropathy (NAION) can present with disc oedema and peripapillary haemorrhage
.However, absence of a history of vasculopathy would warrant further investigation in these patients. Usually, NAION is associated with an absence of pain, however, all the patients in our study over the age of 50 had a subjective absence of pain, again clouding the distinction between the two entities.NAION is usually linked with altitudinal defects on visual field testing
, nevertheless when the presenting VA is too poor to undertake formal visual field testing, then the defect cannot be elucidated. NAION is usually associated with a small or crowded ONH, with an absent cup
, and a consolidating clinical feature would be to examine the optic disc in the contralateral eye to assess if it has a diminished size. Atypical features, involvement of the other eye and a relapsing and remitting should warrant further investigation.
Pain Pain is typically a feature of demyelinating optic neuropathies. The literature states that it is very frequently associated with ON from MS and anti-MOG. It is frequently associated with AQP4 positive ON
. However, an absence of pain does not out rule a demyelinating cause. The 91.67% of our MOG cohort had pain as one of their presenting symptoms while none of our AQP4 cohort reported pain, either periorbital or retrobulbar. Absence of pain in a patient with other signs and symptoms indicative of an ON should be investigated for other cause such as a compressive or space occupying lesion compromising the optic nerve. The vision loss in these patients is usually gradual and progressive
as opposed to the acute or subacute presentations of those with demyelinating lesions.
由于体育教师在高校篮球发展的过程中起着非常关键的作用,因此,高校应该加强培训工作,提升他们的专业技能和综合素质,确保他们能够为篮球运动的发展提供帮助。由于本身具备了比较强的理论知识,但是在实践操作能力上比较缺乏,因此,应该结合各方面的资源推送到实践中进行训练,确保他们能够获得更多的实践性知识,可以帮助学生在体育课上得到更好的吸收。同时,还要加强对体育教师的长久性培训工作和继续教育工作,在有条件的情况之下,还可以输送他们到相应的省队中参加学习,确保他们本身具备较强的教育教学能力,可以提高高校篮球的发展。
78.57% in the affected eye of our MOG cohort had a swollen disc at presentation whereas none of our AQP4 cohort had a swollen disc with 50% of the AQP4 cohort having either a pale disc or normal appearing ONHs. A pale optic disc is usually indicative of a chronic optic nerve condition such as compressive, hereditary, toxic/nutritional optic neuropathies however it can also occur as a sequela of an acute inflammatory or ischemic optic neuropathy
. If the nerve becomes pale secondary to a previous attack of ON, the nerve may not become swollen on repeat attacks highlighting the importance of optic nerve assessment at initial presentation
.One prospective cohort study of patients with ON showed that by testing all cases of ON with bilateral ON, recurrent ON, or optic disc swelling on fundoscopy for MOG antibody, all cases of MOG ON would be detected and only 50% of ON cases in the cohort would be tested overall
.
Relative Afferent Pupillary Defect The presence of a RAPD is a pathognomonic indication of organic disease. In conjunction with a normal retinal examination, it is highly suggestive of optic nerve dysfunction
. However, if pupillary function is brisk and reactive, it does not equate to an absence of an optic nerve disorder. 78.57% of our ant-MOG cohort had a RAPD at presentation. In contrast, only 33.33% of analysed eyes in the anti-AQP4 had an RAPD recorded at presentation.However, these findings need to be taken in conjunction with the clinical context. Two of the eyes which had an absence of an RAPD in the MOG group were a simultaneous bilateral ON with a logMAR VA of 1.0. In this instance, one can assume that both optic nerves are equally dysfunctional and therefore the absolute presence of an RAPD in the MOG cohort could be as high as 92.86%. In the AQP4 group, 2 patients had bilateral simultaneous involvement, but one patient had symptoms of an intranuclear ophthalmoplegia (INO) and brisk pupillary reactions whilst the other had symptoms of consensual optic nerve compromise and therefore the examiner may have had difficulty elucidating an RAPD. Extrapolating from this we can assume that the RAPD incidence at presentation in the AQP4 cohort to be 66.67%.
Subtle RAPDs can be difficult to measure
and so it is essential that if a patient presents with signs and/or symptoms of optic nerve dysfunction and there is a query over the presence of an RAPD that a senior clinician examines the pupillary responses. A patient should never be dilated in the ophthalmic emergency department or the neuro-ophthalmology clinic without the prior confirmation of the presence or absence of this essential ocular finding. If there is optic nerve dysfunction there should
be an RAPD. The verification of this sign will lead the ophthalmologist down specific diagnostic pathways. The presence of an RAPD is nearly always of clinical significance and should always prompt red flags especially in the absence of other ocular or systemic comorbidities
.
Colour Vision and Red Desaturation Many authors argue that colour vision testing is an integral part of assessment of optic nerve functionality
. Multiple difference methods of colour vision testing are available including the Ishihara pseudoisochromic plates, the Hardy-Rand-Rittler test and Farnsworth-Munsell 100 hue test. The most practical and widely used of these is the Ishihara test
which contains 38 plates for testing, but a condensed version of either 10,14 or 24 plates can be used. Ideally these tests are used to screen, classify, and grade severity of colour deficency
but for optic nerve disorders they are used to measure baseline,assess extent, and elicit change in follow up. The results of the tests themselves are dependent on a multitude of patient and environmental factors including lighting, refractive correction, literacy, pre-existing pathology, undiagnosed colour deficiency, cognition
. In our cohort, 85.71% and 66.67%in the MOG and AQP4 group respectively had a deficiency on interpreting the Ishihara plates at presentation. We performed a Pearson correlation between presenting VA and number of plates correctly tested which revealed a moderate positive correlation between the two variables [
(14)=0.5,
=0.002).One can assume that presenting VA is a surrogate marker of colour vision
the worst the presenting VA the fewer plates correctly identified. Some reviews now exclude colour vision testing as a requisite in the neuro ophthalmology exam
unless the examiner is looking to reduce subtle colour defects.In our cohort is the actual VA was 1.0 logMAR units or greater,the number of plates tested correctly was ubiquitously 3 or less and therefore the authors would question the rational of undertaking colour vision testing at this level of vision or worse.Red desaturation is a subjective finding and was assessed in our cohort in a binary fashion. It was present in all but one eye in our MOG cohort (92.86%) and in all eyes that displayed signs of ON in our AQP4 cohort. Red desaturation is a simple,quick, and most importantly a sensitive test for patients with optic nerve disease
. It can be used a surrogate marker of an optic neuropathy as opposed to cumbersome colour vision testing, especially when the presenting VA is poor. However,it is difficult to quantify as it is a subjective test. One study revealed that almost 25% of healthy volunteers, with no documented evidence or ocular or optic nerve disease, stated that they experienced some degree of red desaturation
.
Visual Field Testing 41.67% of our anti-MOG cohort have either improved or unchanged visual field from baseline,while the remaining 16.67% demonstrated a dis-improvement.75% of the patients in our AQP4 cohort showed no change in their visual fields. It has been proposed that anti-AQP4 ON can produce a higher incidence of non-central and altitudinal defects in comparison to MS related ON and that an ischaemic mechanism may underpin this disease
, however these findings were not echoed in our cohort with no altitudinal defects observed. There was a higher incidence of altitudinal defects seen in our MOG cohort with 3 of the 12 eyes (25%)presenting with either a superior or inferior altitudinal defect.The visual field defects in anti-MOG ON tend to be more severe than those seen with MS related ON
.
Visual field testing in ON is used to classify baseline deficit and to monitor change over time. Routinely it is performed at onset if possible and at 3, 6 and 12mo. Visual fields are useful to analyse progression or recovery but due to the wide range of visual fields defects that an ON can produce, it is exceedingly difficult to use pattern of loss to distinguish it from other optic nerve disease. Visual field data extrapolated from the ON treatment trial showed that the most common pattern of loss included diffuse visual field loss in 48%,altitudinal defects in 15% and central or cecocentral scotoma in 8.3%
. There is debate over which type of visual field analyser is the most appropriate for monitoring patients with optic nerve disease with kinetic perimetry, such as the octopus visual field analyser, able to record abnormalities in the far periphery better than the Humphrey visual field analyser(static perimerty). The point was made by Keltner
when they compared kinetic peripheral and central static field in 448 patients in the optic neuritis treatment trial (ONTT)that only 2.9% of affected eye peripheral defects were missed on static perimetry. The authors would argue that this equated to 13 patients that had they visual field results interpreted incorrectly and therefore due to the wide range of visual field defects that ON can produce, kinetic visual fields should be the testing modality of choice.
Magnetic Resonance Imaging MRI can provide clues regarding the aetiology of the demyelination. ON associated with MS is usually displays unilaterality with respect to lesions in the optic nerve and enhancing lesions are frequently seen in the periventricular, subcortical and juxtacortical areas of the brain
. Those positive for anti-AQP4 tend to have to more posterior involvement of the optic nerve including chiasm and simultaneous bilateral disease. These lesions tend to be longer than those seen in MS-ON
. In contrast, the MRI findings in anti-MOG disease tend to have more anterior involvement of the optic nerve sparing the chiasm
, with perineural enhancement of the optic nerve sheath
, but again they tend to be more longitudinally extensive and bilateral in up to 25% of cases
.Only one patient in our MOG group had brain involvement(8.33%) while 100% of this cohort had involvement in their affected nerve on primary MRI. Two of the patients have simultaneous bilateral involvement of the optic nerves(18.67%). In contrast the AQP4 group had more diverse findings, with bilateral optic nerve enhancement extending to the chiasm in one patient, one patient had no evidence of ON and the final patient had nonspecific T2 hyperintensity.
MRI with gadolinium contrast is the gold standard of radiographic imaging for demyelinating disease. All patients should have an MRI brain and optic nerves with contrast preformed. MRI provides high soft tissue contrast and the ability to characterise tissue properties
without exposing the patient to the harmful effects of ionising radiation. The findings in our MOG group are in keeping with what is already in the literature and the findings in the AQP4 group were not in keeping with typical ON and so therefore would warrant further investigation for atypical disease.
据2013年第八个文化遗产日公布,博湖县项目代表性传承人有15人,如此庞大的非遗系统,其代表性传承人屈指可数,这对博湖县非遗的继续发展产生明显的危机。建立非遗保护中心后,博湖县文化馆内6名工作人员和1名分管文化工作的领导具体负责非遗保护工作的落实,几人在6年时间内对博湖县的非遗进行普查、挖掘、保护、传承工作,成绩显著,但在此过程中,缺乏更多人才加入。
Treatment Initial treatment for anti-MOG ON and anti-AQP4 is 1 g per day of intravenous methylprednisolone for 3 to 5d and a slow steroid taper over a period of 1 to 2mo to prevent relapse with steroid withdrawal
. It has been postulated that early intervention with IVMP in these diseases would lead to better long term visual outcomes
however this has not been proven in any prospective randomised trial. There are no clear criteria on the acute treatment for these diseases however we do know that they can present with profound visual loss,tend to relapse and have the tendency to become steroid dependant and therefore high dose steroid emerges to be the initial treatment of choice. The clinician should be careful with the use of high dose steroid especially in the elderly and diabetics. There is no doubt that they have great efficiency in the acute setting however their multitude of side effects warrant careful supervision and deliberate decision making.IVMP has been associated with serious side effects in the acute setting including hepatic insufficiency, avascular necrosis of the femoral head, steroid induced psychosis and autoimmune encephalitis
. The role of plasma exchange remains unclear in Anti-MOG disease whereas there appears to be some benefit in those positive for anti-AQP4
.
All our patients received IVMP 1 g per day for 3 to 5d with an oral prednisolone taper. One patient suffered from steroid induced psychosis and was admitted to a psychiatric hospital for treatment for a short period and subsequently recovered fully with no psychiatric sequalae. In terms of long-term immunosuppression in our cohort, azathioprine was the maintenance medication of choice with 5 of the 12 (41.67%)patients receiving it in the MOG group. Two patients were on methotrexate (16.67%), 1 was taking mycophenolate mofetil (8.33%) and 3 of the remaining 4 (25%; 1 of which was pregnant) were on no maintenance therapy. The final patient was placed on rituximab, underwent plasma exchange and IVIG and maintenance low dose steroid. The 50% of the patients in the AQP4 group either on low dose oral prednisolone or azathioprine. One of our patients in the AQP4 has been subsequently sent for IVIG therapy. Both IVIG and monoclonal antibodies use in these diseases is well documented, but a lack of conclusive evidence exists
.Some medications used in the treatment of multiple sclerosis have proven to be ineffective in treating these atypical cases,particularly anti-MOG related disease. These include interferon beta
, glatiramer acetate
and natalizumab
. There are emerging therapies including the monoclonal antibodies tocilizumab and eculizumab which are both undergoing clinical trials in AQP4 positive patients
. There is a potential role for low dose steroid in conjunction with steroid sparing agents with an increase in the number of relapses observed when prednisolone doses were reduced below 10 mg per day
.
It has been shown that the use of oral and intravenous methylprednisolone to be bioequivalent for the treatment of acute ON
. This may be applicable for those unable to stay in hospital or who live in rural areas and it has shown to be a cost effective measure with a 4d inpatient stay costing a factor of 38 times more than treatment with oral steroid as an outpatient
. However, care should be taken especially with those who may suffer from the side effects of unsupervised high dose steroid administration
frail, elderly, osteoporotic,immunocompromised
The management of optic neuritis has been heavily influenced by the ONTT
, a study which is currently 31 years old.Recent trials have rebutted the inferiority of oral steroid in comparison to intravenous
. This was not tailored towards patients with either anti-MOG or anti-AQP4 related disease and therefore care should be taken when extrapolating treatment and outcome measures from this trial. A recent opinion piece by Petzold
has made a compelling argument for a new corticosteroid treatment trial for acute ON due to vague definitions of symptom onset, delay in initiating treatment and crude outcome measures in the ONTT.
Limitations Limitations of our study included reviewing these patients from an ophthalmic point of view. We only based our cohort of anti-AQP4 positive patients on those who were seropositive and had an episode of ON as opposed to those who met the definition based on the Wingerchuk
’s
criteria. We did not include contrast sensitivity as a measurement of visual dysfunction, which in retrospect would have been an appropriate parameter to record
. We did not include data on cerebrospinal fluid samples and non-ophthalmic morbidity as we believed it to be outside the scope of this article. There was also a wide array of length of follow up ranging from 2 to 131mo. Our patient numbers are relatively low, however due to the paucity of clinical trials on this patient cohort worldwide,we believe that characterising our cohort is important to further classifying these rare disease entities.
In conclusion, our study has shown the range of clinical characteristics that can be associated with both anti-MOG and anti-AQP4 ON. The prompt diagnosis and treatment of these disease is essential to prevent long term ocular sequalae. The role of MRI is essential to delineate disease radiographically.OCT data is proving to be the modality of choice to stratify damage at onset and monitor progression. The role of visual field testing and colour vision testing is equivocal but are adequate subjective indicators of evolution of disease. Further randomised control trials have yet to be carried out to fully clarify most appropriate long terms treatments for these diseases, but work is underway.
ACKNOWLEDGEMENTS
Conflicts of Interest: Murtagh P, None; Coman A, None;Stephenson K, None; Gaughan M, None; Ryan D, None;McNeill G, None; McGuigan C, None; Cassidy L, None.
1 Sato DK, Callegaro D, Lana-Peixoto MA, Waters PJ, de Haidar Jorge FM, Takahashi T, Nakashima I, Apostolos-Pereira SL, Talim N, Simm RF, Lino AMM, Misu T, Leite MI, Aoki M, Fujihara K. Distinction between MOG antibody-positive and AQP4 antibody-positive NMO spectrum disorders.
2014;82(6):474-481.
2 Reindl M, Waters P. Myelin oligodendrocyte glycoprotein antibodies in neurological disease.
2019;15(2):89-102.
3 Jarius S, Wildemann B. Aquaporin-4 antibodies (NMO-IgG) as a serological marker of neuromyelitis optica: a critical review of the literature.
2013;23(6):661-683.
4 Ma XY, Kermode AG, Hu XQ, Qiu W. NMOSD acute attack:Understanding, treatment, and innovative treatment prospect.
2020;348:577387.
5 He D, Li Y, Dai QQ, Zhang YF, Xu Z, Li Y, Cai G, Chu L. Myopathy associated with neuromyelitis optica spectrum disorders.
2016;126(10):863-866.
6 Patterson SL, Goglin SE. Neuromyelitis optica.
2017;43(4):579-591.
7 Sellner J, Boggild M, Clanet M, Hintzen RQ, Illes Z, Montalban X, du Pasquier RA, Polman CH, Sorensen PS, Hemmer B. EFNS guidelines on diagnosis and management of neuromyelitis optica.
2010;17(8):1019-1032.
8 Wingerchuk DM, Lennon VA, Lucchinetti CF, Pittock SJ, Weinshenker BG. The spectrum of neuromyelitis optica.
2007;6(9):805-815.
9 Chen JJ, Flanagan EP, Jitprapaikulsan J, López-Chiriboga AS,Fryer JP, Leavitt JA, Weinshenker BG, McKeon A, Tillema JM,Lennon VA, Tobin WO, Keegan BM, Lucchinetti CF, Kantarci OH,McClelland CM, Lee MS, Bennett JL, Pelak VS, Pittock SJ. Myelin oligodendrocyte glycoprotein antibody-positive optic neuritis: clinical characteristics, radiologic clues, and outcome.
2018;195:8-15.
10 Hyun JW, Woodhall MR, Kim SH, Jeong IH, Kong B, Kim G, Kim Y, Park MS, Irani SR, Waters P, Kim HJ. Longitudinal analysis of myelin oligodendrocyte glycoprotein antibodies in CNS inflammatory diseases.
2017;88(10):811-817.
11 Tajfirouz DA, Bhatti MT, Chen JJ. Clinical characteristics and treatment of MOG-IgG-associated optic neuritis.
2019;19(12):100.
12 Broadway DC. How to test for a relative afferent pupillary defect(RAPD).
2012;25(79-80):58-59.
13 Griffin JF, Wray SH. Acquired color vision defects in retrobulbar neuritis.
1978;86(2):193-201.
14 Jarius S, Ruprecht K, Kleiter I,
, in cooperation with the Neuromyelitis Optica Study Group (NEMOS). MOG-IgG in NMO and related disorders: a multicenter study of 50 patients. Part 1: Frequency,syndrome specificity, influence of disease activity, long-term course,association with AQP4-IgG, and origin.
2016;13(1):279.
15 Costello F, Coupland S, Hodge W, Lorello GR, Koroluk J, Pan YI,Freedman MS, Zackon DH, Kardon RH. Quantifying axonal loss after optic neuritis with optical coherence tomography.
2006;59(6):963-969.
16 Gabilondo I, Martínez-Lapiscina EH, Martínez-Heras E, Fraga-Pumar E, Llufriu S, Ortiz S, Bullich S, Sepulveda M, Falcon C, Berenguer J, Saiz A, Sanchez-Dalmau B, Villoslada P. Trans-synaptic axonal degeneration in the visual pathway in multiple sclerosis.
2014;75(1):98-107.
17 Abel A, McClelland C, Lee MS. Critical review: typical and atypical optic neuritis.
2019;64(6):770-779.
18 Chen JJ, Bhatti MT. Clinical phenotype, radiological features, and treatment of myelin oligodendrocyte glycoprotein-immunoglobulin G(MOG-IgG) optic neuritis.
2020;33(1):47-54.
19 Han S, Jung JJ, Kim US. Differences between non-arteritic anterior ischemic optic neuropathy and open angle glaucoma with altitudinal visual field defect.
2015;29(6):418-423.
20 Doro S, Lessell S. Cup-disc ratio and ischemic optic neuropathy.
1985;103(8):1143-1144.
21 Marzoli SB, Criscuoli A. Pain in optic neuropathies.
2018;39(1):25-31.
22 Behbehani R. Clinical approach to optic neuropathies.
2007;1(3):233-246.
23 O’Neill EC, Danesh-Meyer HV, Kong GXY, Hewitt AW, Coote MA,MacKey DA, Crowston JG, Group ONS. Optic disc evaluation in optic neuropathies: the optic disc assessment project.
2011;118(5):964-970.
24 Ducloyer JB, Caignard A, Aidaoui R, Ollivier Y, Plubeau G, Santos-Moskalyk S, Porphyre L, le Jeune C, Bihl L, Alamine S, Marignier R, Bourcier R, Ducloyer M, Weber M, le Meur G, Wiertlewski S,Lebranchu P. MOG-Ab prevalence in optic neuritis and clinical predictive factors for diagnosis.
2020;104(6):842-845.
25 Cox TA, Thompson HS, Corbett JJ. Relative afferent pupillary defects in optic neuritis.
1981;92(5):685-690.
26 Kawasaki A, Moore P, Kardon RH. Variability of the relative afferent pupillary defect.
1995;120(5):622-633.
27 Strachan K, Jamieson A. The relative afferent pupillary defect: its role in the diagnosis of metastatic malignancy.
2012;105(5):463-466.
28 Chan CKM, Jindahra P, Muñoz S, Robert MP, Pula JH, Vaphiades M. Neuro-ophthalmic literature review.
-
2013;37(4):175-180.
29 Fanlo Zarazaga A, Gutiérrez Vásquez J, Pueyo Royo V. Review of the main colour vision clinical assessment tests.
(
) 2019;94(1):25-32.
30 Birch J. A practical guide for colour-vision examination: report of the Standardization Committee of the International Research Group on Colour-Vision Deficiencies.
1985;5(3):265-285.
31 Petzold A, Wattjes MP, Costello F, Flores-Rivera J, Fraser CL, Fujihara K, Leavitt J, Marignier R, Paul F, Schippling S, Sindic C, Villoslada P,Weinshenker B, Plant GT. The investigation of acute optic neuritis: a review and proposed protocol.
2014;10(8):447-458.
32 Almog Y, Gepstein R, Nemet AY. A simple computer program to quantify red desaturation in patients with optic neuritis.
2014;252(8):1305-1308.
33 Mikolajczyk B, Ritter A, Larson C, Connett J, Olson J, McClelland C,Lee M. Red desaturation prevalence and severity in healthy patients.
2020:10.1212/CPJ.0000000000001011.
34 Nakajima H, Hosokawa T, Sugino M, Kimura F, Sugasawa J, Hanafusa T, Takahashi T. Visual field defects of optic neuritis in neuromyelitis optica compared with multiple sclerosis.
2010;10:45.
35 Vicini R, Brügger D, Abegg M, Salmen A, Grabe HM. Differences in morphology and visual function of myelin oligodendrocyte glycoprotein antibody and multiple sclerosis associated optic neuritis.
2021;268(1):276-284.
36 Keltner J, Johnson C, Spurr J, Beck R. Baseline visual field profile of optic neuritis. The experience of the optic neuritis treatment trial.Optic Neuritis Study Group.
1993;111(2):231-234.
37 Keltner JL, Johnson CA, Spurr JO, Beck RW. Comparison of central and peripheral visual field properties in the optic neuritis treatment trial.
1999;128(5):543-553.
38 Beck RW, Arrington J, Murtagh FR, Cleary PA, Kaufman DI. Brain magnetic resonance imaging in acute optic neuritis. Experience of the Optic Neuritis Study Group.
1993;50(8):841-846.
39 Kim HJ, Paul F, Lana-Peixoto MA, Tenembaum S, Asgari N,Palace J, Klawiter EC, Sato DK, de Seze J, Wuerfel J, Banwell BL,Villoslada P, Saiz A, Fujihara K, Kim SH, Guthy-Jackson Charitable Foundation NMO International Clinical Consortium & Biorepository.MRI characteristics of neuromyelitis optica spectrum disorder: an international update.
2015;84(11):1165-1173.
40 Biotti D, Bonneville F, Tournaire E, Ayrignac X, Dallière CC, Mahieu L, Vignal C, Dulau C, Brochet B, Ruet A, Ouallet JC, Gout O, Heran F, Menjot de Champfleur N, Tourdias T, Deneve M, Labauge P,Deschamps R. Optic neuritis in patients with anti-MOG antibodies spectrum disorder: MRI and clinical features from a large multicentric cohort in France.
2017;264(10):2173-2175.
41 Ramanathan S, Prelog K, Barnes EH,
. Radiological differentiation of optic neuritis with myelin oligodendrocyte glycoprotein antibodies, aquaporin-4 antibodies, and multiple sclerosis.
2016;22(4):470-482.
42 Denève M, Biotti D, Patsoura S,
. MRI features of demyelinating disease associated with anti-MOG antibodies in adults.
2019;46(5):312-318.
43 Grover VPB, Tognarelli JM, Crossey MME, Cox IJ, Taylor-Robinson SD, McPhail MJW. Magnetic resonance imaging: principles and techniques: lessons for clinicians.
2015;5(3):246-255.
44 Stiebel-Kalish H, Hellmann MA, Mimouni M, Paul F, Bialer O, Bach M, Lotan I. Does time equal vision in the acute treatment of a cohort of AQP4 and MOG optic neuritis?
2019;6(4):e572.
45 Walasik-Szemplińska D, Kamiński G, Sudoł-Szopińska I.Life-threatening complications of high doses of intravenous methylprednisolone for treatment of Graves’ orbitopathy.
2019;12:13.
46 Bonnan M, Valentino R, Debeugny S, Merle H, Fergé JL, Mehdaoui H, Cabre P. Short delay to initiate plasma exchange is the strongest predictor of outcome in severe attacks of NMO spectrum disorders.
2018;89(4):346-351.
47 Ramanathan S, Mohammad S, Tantsis E,
, Australasian and New Zealand MOG Study Group. Clinical course, therapeutic responses and outcomes in relapsing MOG antibody-associated demyelination.
2018;89(2):127-137.
48 Jarius S, Ruprecht K, Kleiter I,
, in cooperation with the Neuromyelitis Optica Study Group (NEMOS). MOG-IgG in NMO and related disorders: a multicenter study of 50 patients.Part 2: Epidemiology, clinical presentation, radiological and laboratory features, treatment responses, and long-term outcome.
2016;13(1):280.
49 Hacohen Y, Wong YY, Lechner C,
. Disease course and treatment responses in children with relapsing myelin oligodendrocyte glycoprotein antibody-associated disease.
2018;75(4):478-487.
50 Araki M, Matsuoka T, Miyamoto K, Kusunoki S, Okamoto T, Murata M, Miyake S, Aranami T, Yamamura T. Efficacy of the anti-IL-6 receptor antibody tocilizumab in neuromyelitis optica: a pilot study.
2014;82(15):1302-1306.
51 Pittock SJ, Lennon VA, McKeon A, Mandrekar J, Weinshenker BG,Lucchinetti CF, O'Toole O, Wingerchuk DM. Eculizumab in AQP4-IgG-positive relapsing neuromyelitis optica spectrum disorders: an open-label pilot study.
2013;12(6):554-562.
52 Jurynczyk M, Messina S, Woodhall MR, Raza N, Everett R, Roca-Fernandez A, Tackley G, Hamid S, Sheard A, Reynolds G, Chandratre S, Hemingway C, Jacob A, Vincent A, Leite MI, Waters P, Palace J.Clinical presentation and prognosis in MOG-antibody disease: a UK study.
2017;140(12):3128-3138.
53 Morrow SA, Fraser JA, Day C, Bowman D, Rosehart H,Kremenchutzky M, Nicolle M. Effect of treating acute optic neuritis with bioequivalent oral
intravenous corticosteroids: a randomized clinical trial.
2018;75(6):690-696.
54 Chataway J, Porter B, Riazi A, Heaney D, Watt H, Hobart J, Thompson A. Home versus outpatient administration of intravenous steroids for multiple-sclerosis relapses: a randomised controlled trial.
2006;5(7):565-571.
55 Beck R. The optic neuritis treatment trial.
1988;106(8):1051-1053.
56 le Page E, Veillard D, Laplaud DA, Hamonic S, Wardi R, Lebrun C, Zagnoli F, Wiertlewski S, Deburghgraeve V, Coustans M, Edan G, Investigators C, West Network for Excellence in Neuroscience.Oral
intravenous high-dose methylprednisolone for treatment of relapses in patients with multiple sclerosis (COPOUSEP): a randomised, controlled, double-blind, non-inferiority trial.
2015;386(9997):974-981.
57 Petzold A, Braithwaite T, van Oosten BW, Balk L, Martinez-Lapiscina EH, Wheeler R, Wiegerinck N, Waters C, Plant GT. Case for a new corticosteroid treatment trial in optic neuritis: review of updated evidence.
2020;91(1):9-14.
58 Wingerchuk DM, Lennon VA, Pittock SJ, Lucchinetti CF, Weinshenker BG. Revised diagnostic criteria for neuromyelitis optica.
2006;66(10):1485-1489.
59 Owidzka M, Wilczynski M, Omulecki W. Evaluation of contrast sensitivity measurements after retrobulbar optic neuritis in Multiple Sclerosis.
2014; 252(4):673-677.
猜你喜欢
数学教学通讯·小学版(2022年4期)2022-05-29
少男少女·教育管理(2022年3期)2022-05-12
体育教学(2022年4期)2022-05-05
家园·建筑与设计(2021年14期)2021-11-27
科技研究·理论版(2021年22期)2021-04-18
疯狂英语·新阅版(2019年6期)2019-09-10
科学与财富(2019年11期)2019-08-06
福建基础教育研究(2019年12期)2019-05-28
中国科技纵横(2018年15期)2018-08-29
地震研究(2017年3期)2017-11-06
 International Journal of Ophthalmology2022年7期
International Journal of Ophthalmology2022年7期
- International Journal of Ophthalmology的其它文章
- Impact of OCT scan-patterns in identifying morphological features of lamellar macular holes and macular pseudoholes
- Virtual reality training improves accommodative facility and accommodative range
- Short-term effect of 0.01% atropine sulphate eye gel on myopia progression in children
- Reduced choroidal peripapillary capillaries in thyroidassociated ophthalmopathy with early stage of dysthyroid optic neuropathy
- Incidence of ocular manifestations in patients with graft versus host disease after allogeneic stem cell transplant in Riyadh, Saudi Arabia
- Clinical features, surgical outcomes and genetic analysis of ectodermal dysplasia with ocular diseases